Birmingham Cardio-Renal Group University Hospitals Birmingham University of Birmingham United Kingdom.
Institute of Cardiovascular Sciences University of Birmingham United Kingdom.
J Am Heart Assoc. 2020 Apr 7;9(7):e016041. doi: 10.1161/JAHA.120.016041. Epub 2020 Mar 26.
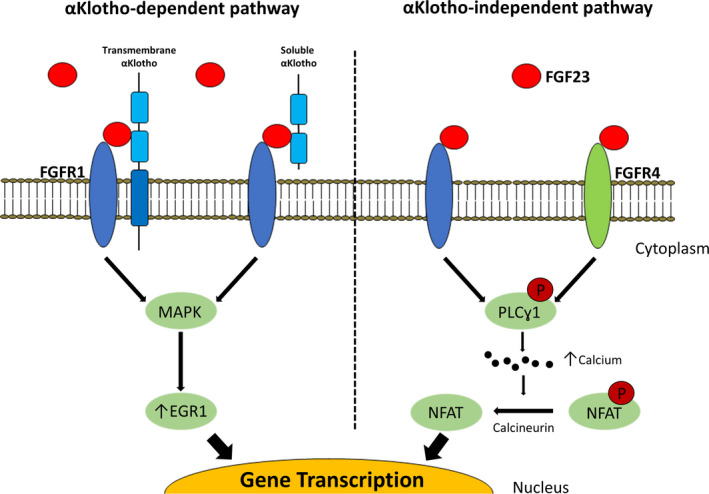
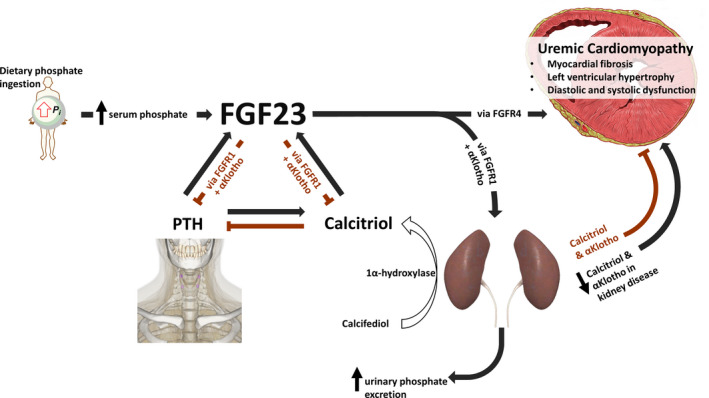
Chronic kidney disease is highly prevalent, affecting 10% to 15% of the adult population worldwide and is associated with increased cardiovascular morbidity and mortality. As chronic kidney disease worsens, a unique cardiovascular phenotype develops characterized by heart muscle disease, increased arterial stiffness, atherosclerosis, and hypertension. Cardiovascular risk is multifaceted, but most cardiovascular deaths in patients with advanced chronic kidney disease are caused by heart failure and sudden cardiac death. While the exact drivers of these deaths are unknown, they are believed to be caused by uremic cardiomyopathy: a specific pattern of myocardial hypertrophy, fibrosis, with both diastolic and systolic dysfunction. Although the pathogenesis of uremic cardiomyopathy is likely to be multifactorial, accumulating evidence suggests increased production of fibroblast growth factor-23 and αKlotho deficiency as potential major drivers of cardiac remodeling in patients with uremic cardiomyopathy. In this article we review the increasing understanding of the physiology and clinical aspects of uremic cardiomyopathy and the rapidly increasing knowledge of the biology of both fibroblast growth factor-23 and αKlotho. Finally, we discuss how dissection of these pathological processes is aiding the development of therapeutic options, including small molecules and antibodies, directly aimed at improving the cardiovascular outcomes of patients with chronic kidney disease and end-stage renal disease.
慢性肾脏病的发病率很高,影响着全球 10%至 15%的成年人,与心血管发病率和死亡率的增加有关。随着慢性肾脏病的恶化,会出现一种独特的心血管表型,其特征为心肌疾病、动脉僵硬增加、动脉粥样硬化和高血压。心血管风险是多方面的,但在晚期慢性肾脏病患者中,大多数心血管死亡是由心力衰竭和心源性猝死引起的。虽然这些死亡的确切原因尚不清楚,但据信是由尿毒症性心肌病引起的:一种心肌肥厚、纤维化的特定模式,伴有舒张和收缩功能障碍。尽管尿毒症性心肌病的发病机制可能是多因素的,但越来越多的证据表明,成纤维细胞生长因子-23 的产生增加和 αKlotho 缺乏是尿毒症性心肌病患者心脏重构的潜在主要驱动因素。本文综述了对尿毒症性心肌病的生理学和临床方面的理解的不断加深,以及对成纤维细胞生长因子-23 和 αKlotho 生物学的快速增加的认识。最后,我们讨论了如何剖析这些病理过程,以帮助开发治疗选择,包括针对改善慢性肾脏病和终末期肾病患者心血管结局的小分子和抗体。