Independent Researcher, Kigali, Rwanda.
Department of Health Studies, College of Human Sciences, University of South Africa, Pretoria, South Africa.
PLoS One. 2020 Apr 2;15(4):e0230478. doi: 10.1371/journal.pone.0230478. eCollection 2020.
Approximately one-third of the global stillbirth burden occurs during intrapartum period. The ability to assess obstetric parameters including effacement, dilatation, uterine contraction, decent, rupture of the uterus, and moulding of the foetal head are among the essential competencies required by obstetric service providers admitting women for labour in health facilities. Misdiagnosis of these conditions could result in unnecessary obstetric interventions and unfavourable obstetric outcomes including intrapartum stillbirth. This study aimed to assess associations between missed diagnosis plus complication of labour on admission and intrapartum stillbirth.
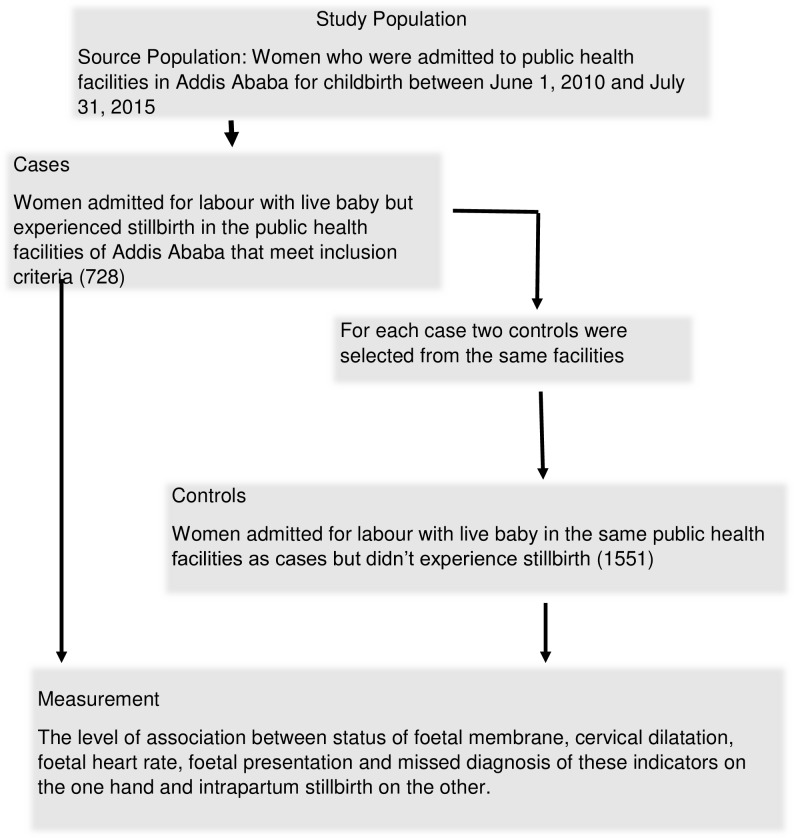
A case-control study using primary data from chart review of medical records of women who experienced intrapartum stillbirth in 20 public health centres and three public hospitals of Addis Ababa between 01 July 2010 and 30 June 2015 was conducted. Data were collected from charts of all cases meeting the inclusion criteria. Medical records of women with livebirths were randomly selected and reviewed from each public health facilities in two to one (2:1) control to case ratio. Accordingly, 728 cases of stillbirth out of 1,056 charts met the inclusion criteria whereas 1,551 controls out of 1,705 were also considered in the study.
Proportionally, more women in the stillbirth group (39.4%) than in the livebirth group (30.2%) experienced ruptured membrane on admission, with the difference being statistically significant (OR 1.7, 95% CI 1.37-2.03). Significantly higher proportion of women in the intrapartum stillbirth group experienced FRH lower than 110/min, a result suggestive of foetal distress on admission. Proportionally, more women in the intrapartum stillbirth group (14.5%) than in the livebirth group (4.5%) had breech foetal presentation on admission for labour, the difference being statistically significant (aOR 3.26 95% CI 1.93-5.50). Intrapartum stillbirth was slightly higher among women with cervical dilatation 4cm or more on admission (OR 1.2, 95% CI 1.00-1.45). This could be owing to delay in seeking obstetric care or misdiagnosis of the condition, a situation that seeks more rigorous study to determine the underlying causal links. Diagnosis of foetal member was missed among more cases than controls where the difference was statistically significant (aOR 1.51, CI 1.03-2.19).
Low FHR, non-vertex foetal presentations and ruptured cervical membrane were predictors of intrapartum stillbirth. Health facilities could avert unnecessary foetal loss by undertaking timely actions to manage obstetric emergencies on admission to labour.
全球约三分之一的死产发生在分娩期间。评估产科参数的能力,包括子宫颈消失、扩张、子宫收缩、胎先露下降、子宫破裂和胎头塑形,是产科服务提供者在医疗机构为产妇分娩时所需的基本能力之一。这些情况的误诊可能导致不必要的产科干预和不良的产科结局,包括分娩期死产。本研究旨在评估入院时漏诊和产时并发症与分娩期死产之间的关系。
这是一项病例对照研究,使用了 2010 年 7 月 1 日至 2015 年 6 月 30 日期间在亚的斯亚贝巴的 20 个公共卫生中心和 3 家公立医院经历分娩期死产的妇女的病历回顾的原始数据。从所有符合纳入标准的病例的图表中收集数据。从每个公共卫生设施中随机选择并审查有活产的妇女的病历,按照 2:1 的比例进行病例对照。因此,在 1056 份图表中,有 728 份符合纳入标准的死产病例,而 1705 份中有 1551 份对照病例也被纳入研究。
在死产组中,更多的妇女(39.4%)在入院时经历了胎膜破裂,而在活产组中,这一比例为 30.2%,差异具有统计学意义(OR 1.7,95%CI 1.37-2.03)。在分娩期死产组中,有更高比例的妇女(14.5%)在入院时出现胎心率(FHR)低于 110/min,这表明入院时胎儿有窘迫的迹象。在入院时的胎位中,死产组中更多的妇女(14.5%)为臀位,而活产组中这一比例为 4.5%,差异具有统计学意义(aOR 3.26,95%CI 1.93-5.50)。在入院时宫颈扩张 4cm 或以上的妇女中,分娩期死产的发生率略高(OR 1.2,95%CI 1.00-1.45)。这可能是由于寻求产科护理的时间延迟或对病情的误诊,需要更严格的研究来确定潜在的因果关系。在病例组中,漏诊胎儿肢体的比例高于对照组,差异具有统计学意义(aOR 1.51,CI 1.03-2.19)。
低胎心率、非头位胎儿和胎膜破裂是分娩期死产的预测因素。医疗机构可以通过及时采取行动来管理入院时的产科急症,从而避免不必要的胎儿死亡。