Department of Cardiology, National University Heart Centre, Singapore, Singapore.
Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore.
Sci Rep. 2020 Apr 22;10(1):6799. doi: 10.1038/s41598-020-63825-8.
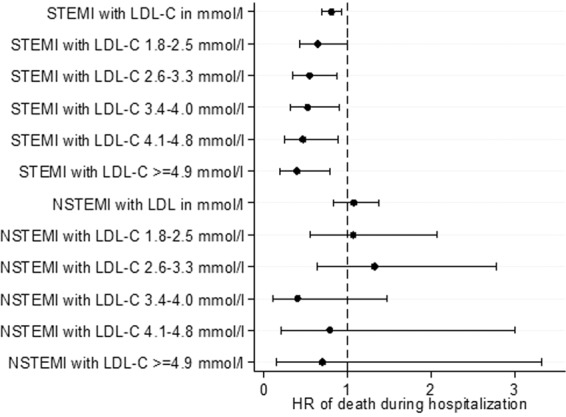
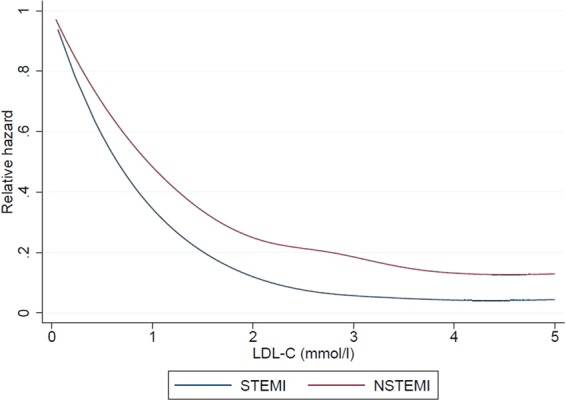
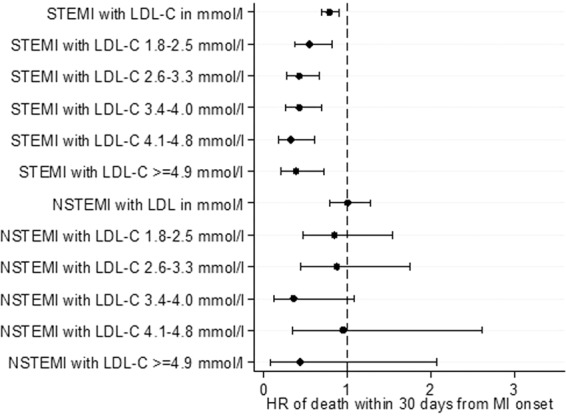
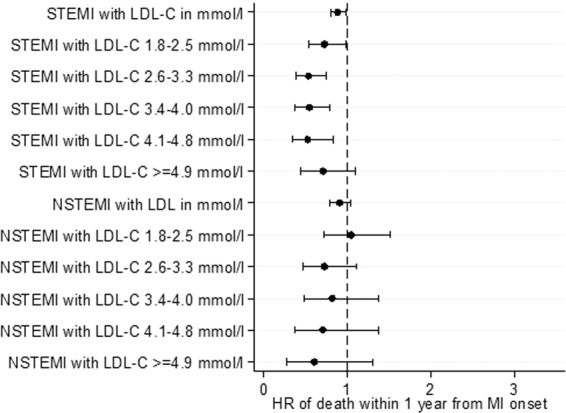
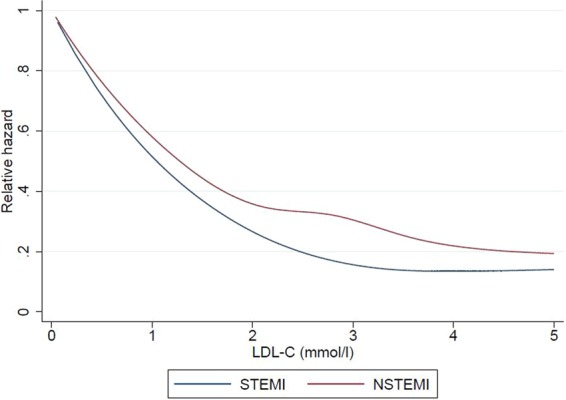
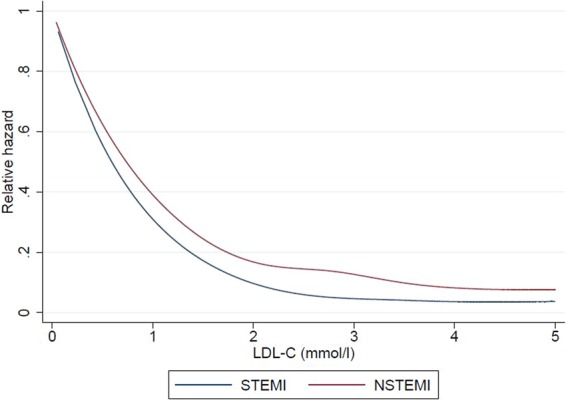
Lowering low-density lipoprotein (LDL-C) and triglyceride (TG) levels form the cornerstone approach of cardiovascular risk reduction, and a higher high-density lipoprotein (HDL-C) is thought to be protective. However, in acute myocardial infarction (AMI) patients, higher admission LDL-C and TG levels have been shown to be associated with better clinical outcomes - termed the 'lipid paradox'. We studied the relationship between lipid profile obtained within 72 hours of presentation, and all-cause mortality (during hospitalization, at 30-days and 12-months), and rehospitalization for heart failure and non-fatal AMI at 12-months in ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI) patients treated by percutaneous coronary intervention (PCI). We included 11543 STEMI and 8470 NSTEMI patients who underwent PCI in the Singapore Myocardial Infarction Registry between 2008-2015. NSTEMI patients were older (60.3 years vs 57.7 years, p < 0.001) and more likely to be female (22.4% vs 15.0%, p < 0.001). In NSTEMI, a lower LDL-C was paradoxically associated with worse outcomes for death during hospitalization, within 30-days and within 12-months (all p < 0.001), but adjustment eliminated this paradox. In contrast, the paradox for LDL-C persisted for all primary outcomes after adjustment in STEMI. For NSTEMI patients, a lower HDL-C was associated with a higher risk of death during hospitalization but in STEMI patients a lower HDL-C was paradoxically associated with a lower risk of death during hospitalization. For this endpoint, the interaction term for HDL-C and type of MI was significant even after adjustment. An elevated TG level was not protective after adjustment. These observations may be due to differing characteristics and underlying pathophysiological mechanisms in NSTEMI and STEMI.
降低低密度脂蛋白(LDL-C)和甘油三酯(TG)水平是降低心血管风险的基础方法,而较高的高密度脂蛋白(HDL-C)被认为是具有保护作用的。然而,在急性心肌梗死(AMI)患者中,较高的入院时 LDL-C 和 TG 水平与更好的临床结局相关,这种现象被称为“血脂悖论”。我们研究了在经皮冠状动脉介入治疗(PCI)的 ST 段抬高型心肌梗死(STEMI)和非 ST 段抬高型心肌梗死(NSTEMI)患者就诊后 72 小时内获得的血脂谱与全因死亡率(住院期间、30 天和 12 个月时)以及心力衰竭和非致命性 AMI 的再住院之间的关系。我们纳入了 2008 年至 2015 年间在新加坡心肌梗死登记处接受 PCI 的 11543 例 STEMI 和 8470 例 NSTEMI 患者。NSTEMI 患者年龄较大(60.3 岁 vs 57.7 岁,p<0.001),且更可能为女性(22.4% vs 15.0%,p<0.001)。在 NSTEMI 中,LDL-C 降低与住院期间、30 天内和 12 个月内的死亡风险增加相关(均 p<0.001),但调整后消除了这种悖论。相反,调整后 STEMI 患者的所有主要结局仍存在 LDL-C 悖论。对于 NSTEMI 患者,较低的 HDL-C 与住院期间死亡风险增加相关,但对于 STEMI 患者,较低的 HDL-C 与住院期间死亡风险降低相关。对于这一终点,即使在调整后,HDL-C 和 MI 类型的交互项仍然具有统计学意义。调整后,TG 水平升高并没有保护作用。这些观察结果可能归因于 NSTEMI 和 STEMI 之间不同的特征和潜在的病理生理机制。