Aygün Nurcihan, Uludağ Mehmet
Department of General Surgery, Health Sciences University, Sisli Hamidiye Etfal Training and Research Hospital, Istanbul, Turkey.
Sisli Etfal Hastan Tip Bul. 2019 Aug 27;53(3):201-214. doi: 10.14744/SEMB.2019.56873. eCollection 2019.
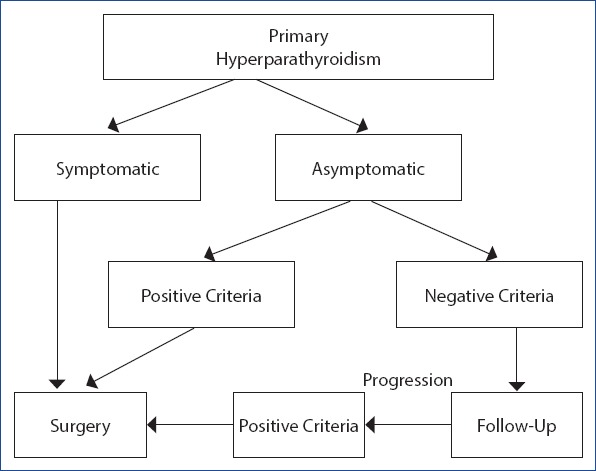
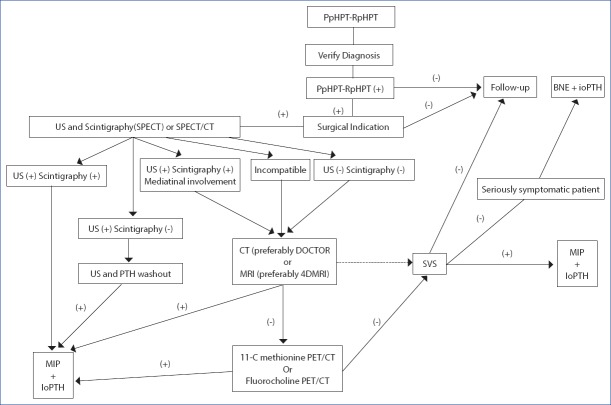
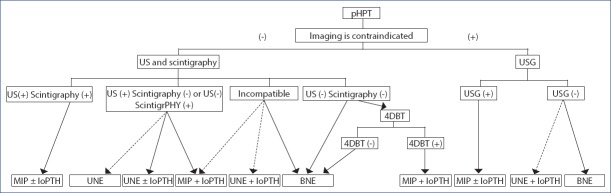
Primary hyperparathyroidism (pHPT) is characterized by an increase in the levels of PTH and Ca, or one of these (Ca, PTH) as a result of a dysregulation of calcium (Ca) metabolism due to inappropriate excess parathyroid hormone (PTH) autonomously produced from one or more than one parathyroid glands. Ninety to 95% of pHPT is a sporadic type, which is not associated with the familial history and other endocrine organ tumors, and 5-10% of it is hereditary. While 80-85% of pHPT arises from a single parathyroid adenoma, 4-5% is caused by a double adenoma, 10-15% by multigland hyperplasia and less than 1% by parathyroid cancer. The diagnosis of pHPT is reached biochemically. The only curative treatment of pHPT is surgery. The choice of surgery in pHPT may vary depending on whether the patient has hereditary HPT or thyroid disease requiring surgical treatment, preoperative localization studies and the findings in these studies, the possibilities of using intraoperative PTH and the preference of the surgeon. The preoperatively determined surgical strategy can be revised according to intraoperative findings in case of need to achieve excellent results. The two main approaches in the surgical treatment of pHPT are BNE (bilateral neck exploration) and MIP (minimal invasive parathyroidectomy). Although BNE is a consistently valid option that has excellent results in the surgical treatment of pHPT and is considered the gold standard, MIP is the ideal approach in selected patients with clinically and radiologically considered a single-gland disease. Negative imaging is not a contraindication for parathyroid surgery and is not a criterion for the presence or absence of surgical indication. Although both methods are safe and effective in the surgical treatment of sporadic pHPT, there is still controversy regarding the effectiveness of both methods. Surgical intervention should establish the risk-benefit balance well, minimize the risk of persistent and recurrent disease and provide the highest cure rate without increasing the risk of complications. Complication rates are higher in the secondary surgery, thus in secondary procedures, selective surgery should be performed under guidance of an imaging modality. The surgical strategy should be determined to achieve maximum cure with minimum dissection and minimal morbidity. In this study, we aimed to determine the type of surgical treatment and pHPT patients suitable for the surgical treatment.
原发性甲状旁腺功能亢进症(pHPT)的特征是甲状旁腺激素(PTH)和血钙水平升高,或因一个或多个甲状旁腺自主分泌过量甲状旁腺激素(PTH)导致钙代谢失调,从而出现PTH和血钙水平升高,或仅其中一项升高。90%至95%的pHPT为散发性,与家族病史及其他内分泌器官肿瘤无关,5%至10%为遗传性。80%至85%的pHPT由单个甲状旁腺腺瘤引起,4%至5%由双腺瘤引起,10%至15%由多腺体增生引起,不到1%由甲状旁腺癌引起。pHPT的诊断依靠生化检查。pHPT唯一的治愈性治疗方法是手术。pHPT的手术选择可能因患者是否患有遗传性甲状旁腺功能亢进症或需要手术治疗的甲状腺疾病、术前定位研究及其结果、术中使用PTH的可能性以及外科医生的偏好而有所不同。如有必要,为取得良好效果,可根据术中发现对术前确定的手术策略进行调整。pHPT手术治疗的两种主要方法是双侧颈部探查(BNE)和微创甲状旁腺切除术(MIP)。尽管BNE是一种始终有效的选择,在pHPT手术治疗中效果良好,被视为金标准,但MIP是临床和影像学检查认为是单腺体疾病的特定患者的理想治疗方法。阴性影像学检查并非甲状旁腺手术的禁忌证,也不是有无手术指征的标准。虽然这两种方法在散发性pHPT手术治疗中均安全有效,但关于两种方法的有效性仍存在争议。手术干预应妥善权衡风险与收益,将持续性和复发性疾病的风险降至最低,并在不增加并发症风险的情况下提供最高治愈率。二次手术的并发症发生率较高,因此在二次手术中,应在影像学检查的指导下进行选择性手术。应确定手术策略,以在最小限度的解剖和最低的发病率下实现最大程度的治愈。在本研究中,我们旨在确定手术治疗的类型以及适合手术治疗的pHPT患者。