Key Laboratory of Pediatric Hematology and Oncology Ministry of Health, Department of Hematology & Oncology, Shanghai Children's Medical Center, School of Medicine, Shanghai Jiao Tong University, Shanghai, China.
J Cell Mol Med. 2020 Jun;24(12):6704-6715. doi: 10.1111/jcmm.15322. Epub 2020 May 11.
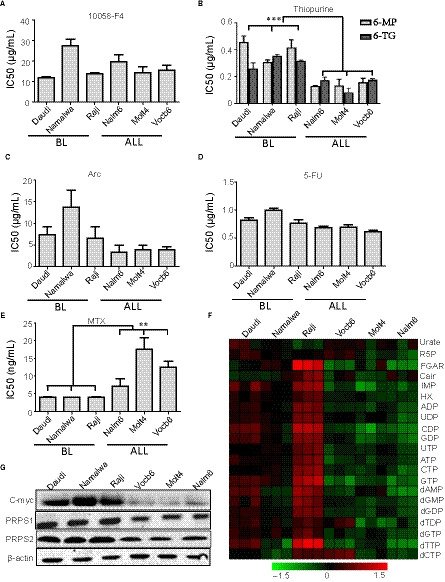
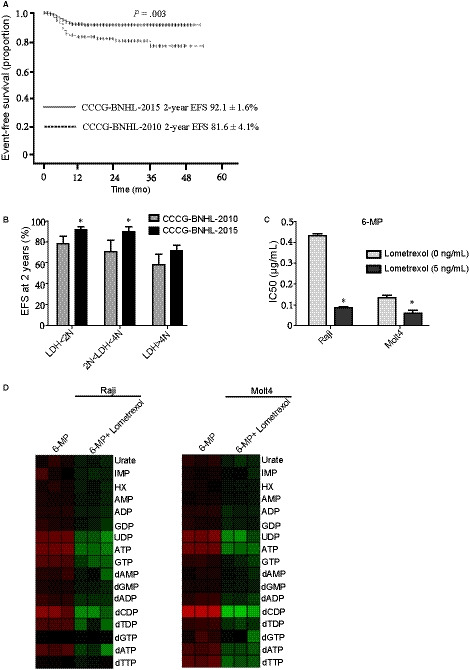
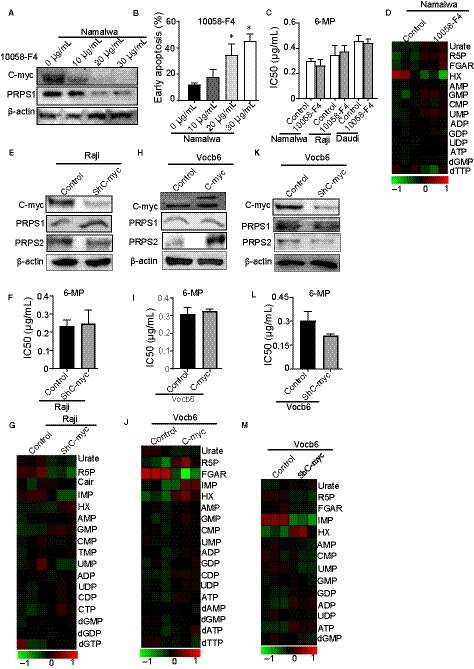
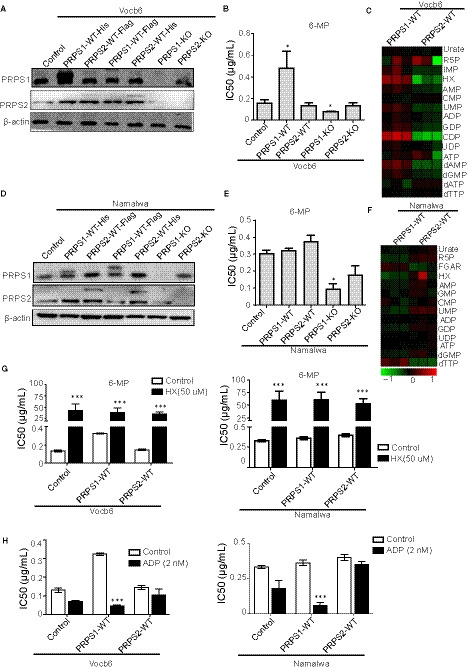
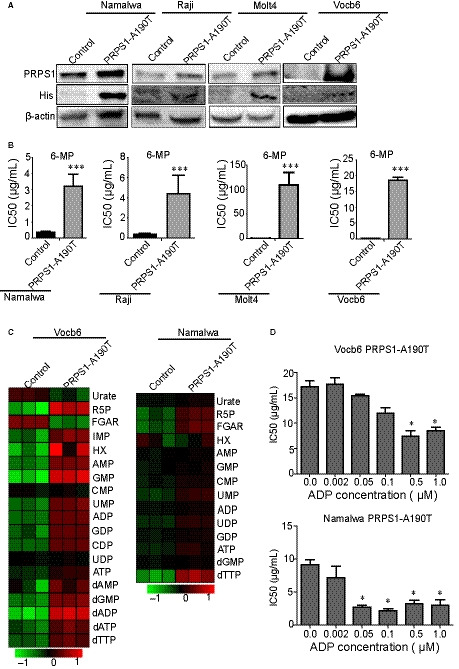
Patients with relapsed/refractory Burkitt's lymphoma (BL) have a dismal prognosis. Current research efforts aim to increase cure rates by identifying high-risk patients in need of more intensive or novel therapy. The 8q24 chromosomal translocation of the c-Myc gene, a main molecular marker of BL, is related to the metabolism by regulating phosphoribosyl pyrophosphate synthetase 2 (PRPS2). In our study, BL showed significant resistance to thiopurines. PRPS2 homologous isoenzyme, PRPS1, was demonstrated to play the main role in thiopurine resistance. c-Myc did not have direct effects on thiopurine resistance in BL for only driving PRPS2. PRPS1 wild type (WT) showed different resistance to 6-mercaptopurine (6-mp) in different metabolic cells because it could be inhibited by adenosine diphosphate or guanosine diphosphate negative feedback. PRPS1 A190T mutant could dramatically increase thiopurine resistance in BL. The interim analysis of the Treatment Regimen for Children or Adolescent with mature B cell non-Hodgkin's lymphoma in China (CCCG-B-NHL-2015 study) confirms the value of high-dose methotrexate (MTX) and cytarabine (ARA-C) in high-risk paediatric patients with BL. However, there remains a subgroup of patients with lactate dehydrogenase higher than four times of the normal value (4N) for whom novel treatments are needed. Notably, we found that the combination of thiopurines and the phosphoribosylglycinamide formyltransferase (GART) inhibitor lometrexol could serve as a therapeutic strategy to overcome thiopurine resistance in BL.
复发/难治性伯基特淋巴瘤 (BL) 患者预后不良。目前的研究旨在通过识别需要更强化或新型治疗的高危患者来提高治愈率。c-Myc 基因 8q24 染色体易位是 BL 的主要分子标志物,与通过调节磷酸核糖焦磷酸合成酶 2 (PRPS2) 的代谢有关。在我们的研究中,BL 对硫嘌呤表现出明显的耐药性。PRPS2 同工酶 PRPS1 被证明在硫嘌呤耐药中起主要作用。c-Myc 对 BL 中的硫嘌呤耐药没有直接影响,因为它仅驱动 PRPS2。PRPS1 野生型 (WT) 在不同代谢细胞中对 6-巯基嘌呤 (6-mp) 表现出不同的耐药性,因为它可以被腺苷二磷酸或鸟苷二磷酸负反馈抑制。PRPS1 A190T 突变体可显著增加 BL 中的硫嘌呤耐药性。中国儿童和青少年成熟 B 细胞非霍奇金淋巴瘤治疗方案(CCCG-B-NHL-2015 研究)的中期分析证实了大剂量甲氨蝶呤 (MTX) 和阿糖胞苷 (ARA-C) 在高危 BL 儿科患者中的价值。然而,仍有一部分患者的乳酸脱氢酶高于正常值的四倍 (4N),需要新的治疗方法。值得注意的是,我们发现硫嘌呤与磷酸核糖甘氨酰胺 formyltransferase (GART) 抑制剂洛美曲索联合使用可能成为克服 BL 硫嘌呤耐药的治疗策略。