Department of Oncology-Pathology, Karolinska Institute and University Hospital Solna, Stockholm, Sweden.
Cancer Centrum Karolinska, CCK, Plan 00, Visionsgatan 56, Karolinska Universitetssjukhuset, Solna, 17164, Stockholm, Sweden.
BMC Cancer. 2020 May 18;20(1):440. doi: 10.1186/s12885-020-06925-y.
After neoadjuvant chemotherapy of breast cancer pathologic complete response (pCR) indicates a favorable prognosis. Among non-selected patients, pCR is, however, achieved in only 10-30%. Early evaluation of tumour response to treatment would facilitate individualized therapy, with ineffective chemotherapy interrupted or changed. The methodology for this purpose is still limited. Tumour imaging and analysis of macromolecules, released from disrupted tumour cells, are principal alternatives.
To investigate whether a metric of cell-loss, defined as the ratio between serum concentration of thymidine kinase1 (sTK1, ng x ml) and tumour volume, can be used for early prediction of pathologic response.
One hunred four women with localized breast cancer received neoadjuvant epirubicin/docetaxel in 6 cycles, supplemented with bevacizumab in cycles 3-6. The cell-loss metric was established at baseline (n = 104), 48 h after cycle 2 (n = 104) and prior to cycle 2 (n = 57). The performance of the metric was evaluated by association with pathologic tumour response at surgery 4 months later.
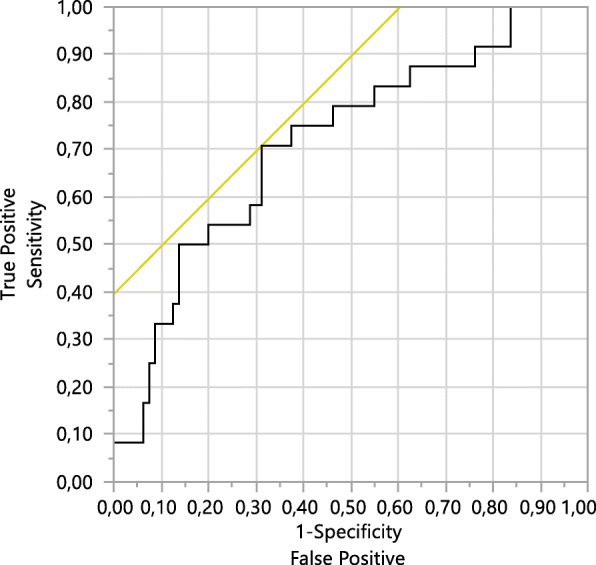
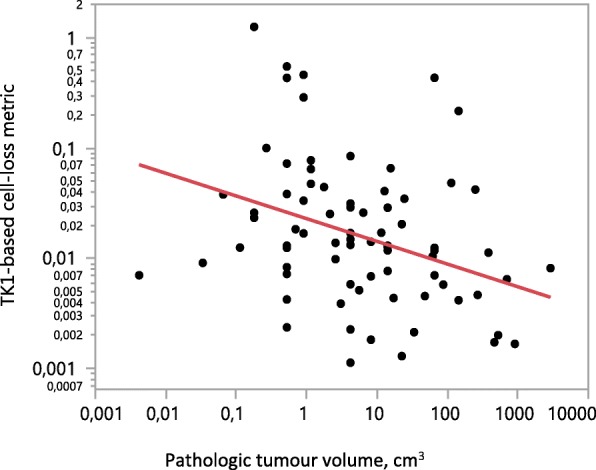
Treatment caused a rise in sTK1, a reduction in tumour volume and a marked increase in the cell-loss metric. Patients were subdivided into quartiles according to the baseline cell-loss metric. For these groups, baseline means were 0.0016, 0.0042, 0.0062, 0.0178 units. After subtraction of baselines, means for the quartiles 48 h after treatment 2 were 0.002, 0.011, 0.030 and 0.357 units. pCR was achieved in 24/104, their distribution in the quartiles (11, 11, 23 and 46%) differed significantly (p = 0.01). In 80 patients with remaining tumour, tumour size was inversely related to the metric (p = 0.002). In 57 patients studied before treatment 2, positive and negative predictive values of the metric were 77.8 and 83.3%, compared to 40.5 and 88.7% 48 h after treatment 2.
A cell-loss metric, based on serum levels of TK1, released from disrupted tumour cells, and tumour volume, reveal tumour response early during neoadjuvant treatment. The metric reflect tumour properties that differ greatly between patients and determine the sensitivity to cytotoxic treatment. The findings point to the significance of cell loss for tumour growth rate. The metric should be considered in personalized oncology and in the evaluation of new therapeutic modalities.
PROMIX (Clinical Trials.govNCT000957125).
乳腺癌新辅助化疗后病理完全缓解(pCR)表明预后良好。然而,在未经选择的患者中,pCR 仅达到 10-30%。早期评估肿瘤对治疗的反应将有助于个体化治疗,中断或改变无效的化疗。为此目的的方法仍然有限。肿瘤成像和分析从受损肿瘤细胞释放的大分子是主要的替代方法。
研究细胞丢失的度量标准,定义为血清胸苷激酶 1(sTK1)浓度与肿瘤体积的比值,是否可用于早期预测病理反应。
104 名患有局限性乳腺癌的女性接受了 6 个周期的表柔比星/多西他赛新辅助治疗,并在第 3-6 个周期中补充贝伐珠单抗。在基线(n=104)、第 2 周期后 48 小时(n=104)和第 2 周期前(n=57)建立细胞丢失度量标准。通过与 4 个月后手术时的病理肿瘤反应相关联来评估该度量标准的性能。
治疗引起 sTK1 升高、肿瘤体积缩小和细胞丢失度量标准明显增加。根据基线细胞丢失度量标准,患者被分为四分之一。对于这些组,基线平均值分别为 0.0016、0.0042、0.0062、0.0178 单位。在减去基线后,第 2 个周期后 48 小时的四分位数平均值分别为 0.002、0.011、0.030 和 0.357 单位。104 例患者中有 24 例获得 pCR,其分布在四分位数(11、11、23 和 46%)中差异显著(p=0.01)。在 80 例仍有肿瘤的患者中,肿瘤大小与该指标呈反比关系(p=0.002)。在 57 例在第 2 个周期前接受治疗的患者中,该指标的阳性和阴性预测值分别为 77.8%和 83.3%,而第 2 个周期后 48 小时的阳性和阴性预测值分别为 40.5%和 88.7%。
基于从受损肿瘤细胞释放的 TK1 血清水平和肿瘤体积的细胞丢失度量标准,可在新辅助治疗期间早期发现肿瘤反应。该指标反映了患者之间差异很大的肿瘤特性,并决定了对细胞毒性治疗的敏感性。这些发现表明细胞丢失对肿瘤生长速度的重要性。该指标应在肿瘤个体化治疗和新治疗方法的评估中考虑。
PROMIX(ClinicalTrials.govNCT000957125)。