Kumar S, Diamond T
Basic Physician Trainee, Northern Sydney Coastal Network, Sydney, Australia.
St George Public Hospital, Kogarah, NSW 2217, Australia.
Bone Rep. 2020 May 6;12:100276. doi: 10.1016/j.bonr.2020.100276. eCollection 2020 Jun.
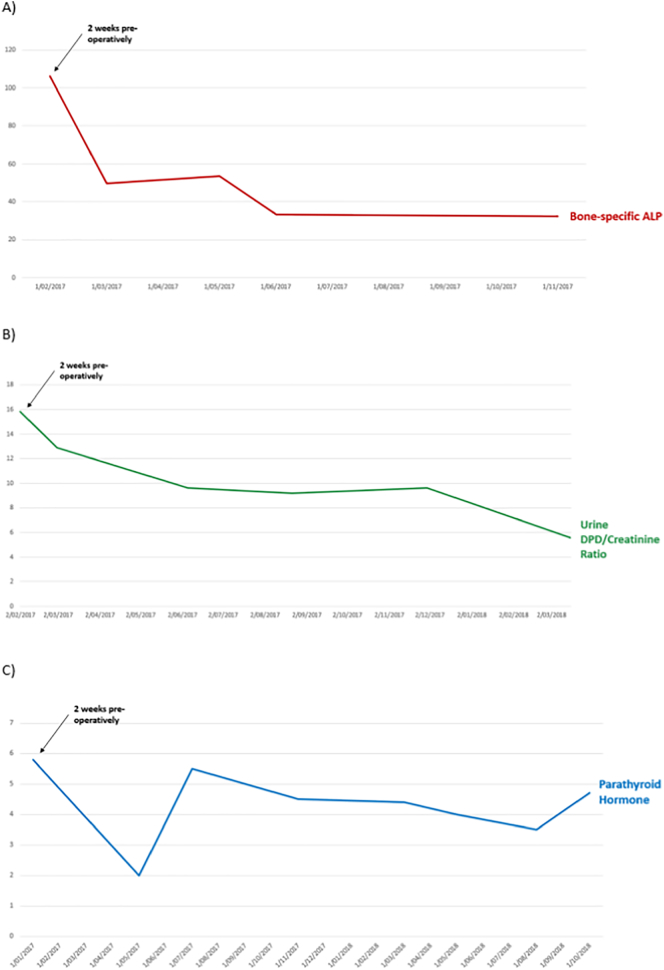
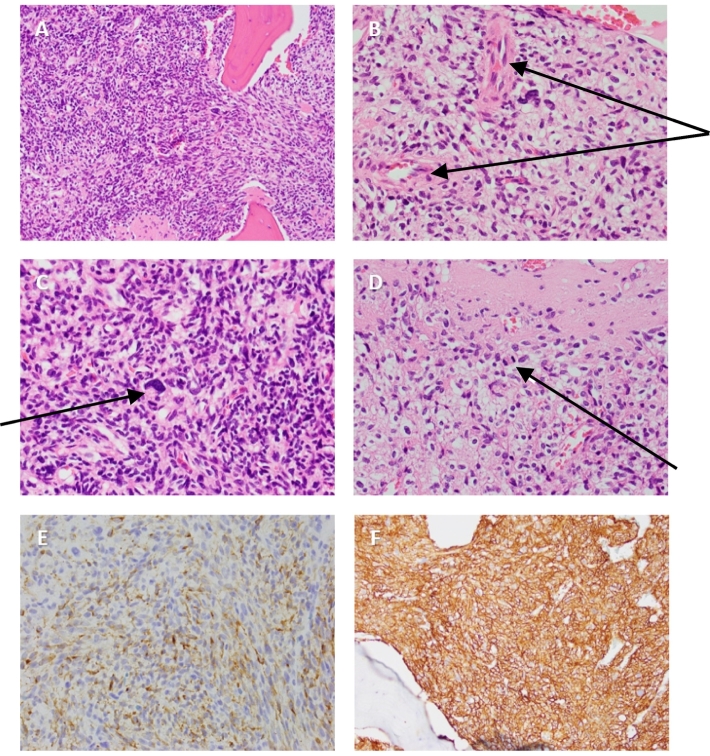
Tumour-induced osteomalacia (TIO) is a rare paraneoplastic syndrome caused by a fibroblast growth-factor-23 (FGF-23)-secreting phosphaturic mesenchymal tumour (PMT) and is characterised by hypophosphataemic osteomalacia. We present a 36-year-old man initially presenting with diffuse bone and joint pain who was inappropriately treated for presumed ankylosing spondylitis for 2 years. Whole-body bone scan suggested metabolic bone disease, prompting referral to our endocrine institution. He was subsequently diagnosed with persistent hypophosphataemia, inappropriately high renal tubular phosphate excretion, 1,25-dihydroxyvitamin D suppression, severe osteoporosis and severe osteomalacia. FGF-23 concentrations (140 ng/L) were raised 3-fold above the upper limit of normal. Initial Gallium-68 (Ga) DOTATATE positron emission tomography (PET)/CT scan missed an active lesion in the left fibular head as the field only included the mid-brain to the proximal femora. Histopathology results from tumour resection confirmed a PMT over-expressing FGF-23. Serum phosphate and FGF-23 normalised immediately post-operatively. He developed severe hypocalcaemia 3-weeks post-operatively (1.77 mmol/L) which normalised after 1 month of high-dose caltrate and calcitriol therapy. Osteomalacia, osteoporosis and associated symptoms resolved during medium-term follow-up with >100% improvement in his bone mineral density. This case report and discussion highlights the pitfalls contributing to delayed diagnosis of TIO and alerts clinicians to the potential complication of hungry bone syndrome post-tumour resection.
肿瘤诱导的骨软化症(TIO)是一种罕见的副肿瘤综合征,由分泌成纤维细胞生长因子23(FGF-23)的磷酸尿性间叶肿瘤(PMT)引起,其特征为低磷性骨软化症。我们报告一名36岁男性,最初表现为弥漫性骨和关节疼痛,因疑似强直性脊柱炎接受了2年的不恰当治疗。全身骨扫描提示代谢性骨病,促使其转诊至我们的内分泌机构。随后他被诊断为持续性低磷血症、肾小管磷排泄过高、1,25-二羟维生素D受抑制、严重骨质疏松和严重骨软化症。FGF-23浓度(140 ng/L)比正常上限升高了3倍。最初的镓-68(Ga) DOTATATE正电子发射断层扫描(PET)/CT扫描遗漏了左腓骨头的一个活性病灶,因为扫描范围仅包括中脑至股骨近端。肿瘤切除的组织病理学结果证实为一个过度表达FGF-23的PMT。术后血清磷和FGF-23立即恢复正常。术后3周他出现严重低钙血症(1.77 mmol/L),在接受1个月的高剂量钙尔奇和骨化三醇治疗后恢复正常。在中期随访期间,骨软化症、骨质疏松症及相关症状得到缓解,骨密度改善超过100%。本病例报告及讨论强调了导致TIO诊断延迟的陷阱,并提醒临床医生注意肿瘤切除后饥饿骨综合征的潜在并发症。