From the Departments of Pediatrics (E.I.P., R.S.Z., W.P.M., A.O.G., T.C.L., P.J.O., J.B.E.), Radiology (D.R.N.), Bioinformatics and Biostatistics Core (R.S.), and Neurology (D.L.K.-J.), University of Minnesota, Minneapolis; and Sangamo Therapeutics (W.P.M.), Richmond, CA.
Neurology. 2020 Aug 4;95(5):e591-e600. doi: 10.1212/WNL.0000000000009929. Epub 2020 Jul 2.
To quantify benchmark treatment outcomes that may be enabled by newborn screening surveillance for X-linked adrenoleukodystrophy (ALD), we report neurocognitive, neuropsychiatric, and MRI change for boys who underwent hematopoietic stem cell transplant (HSCT) at initial stages of demyelination, prior to neurocognitive signs of disease.
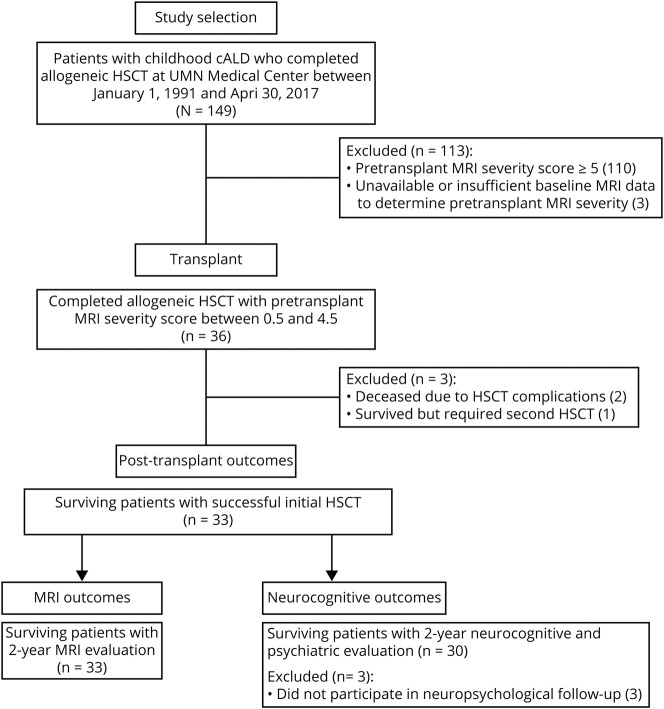
Retrospective chart review identified 36 patients whose cerebral ALD was detected and treated early, with lesion severity less than 5 on the ALD-specific MRI scoring system. Median age at transplant was 7.3 years (range, 4.0-16.1). Progression of radiologic disease on MRI in the 2 years following HSCT was examined relative to the severity of the initial lesion for 33 patients, and longitudinal neurocognitive and neuropsychiatric outcomes were studied for 30 patients.
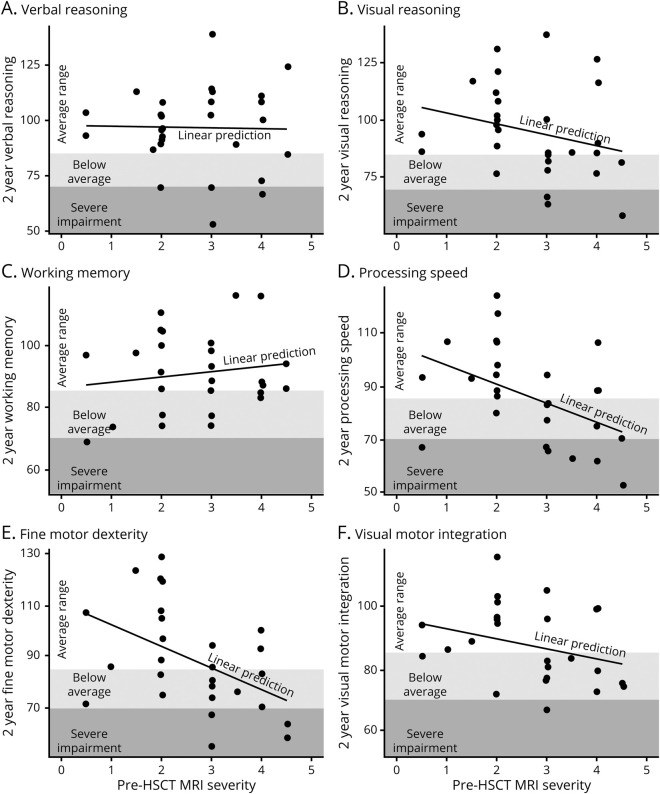
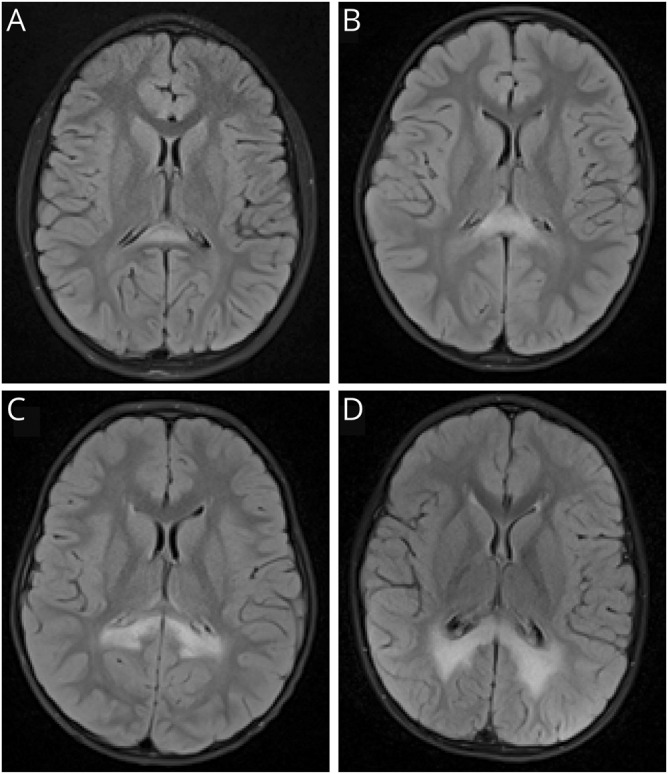
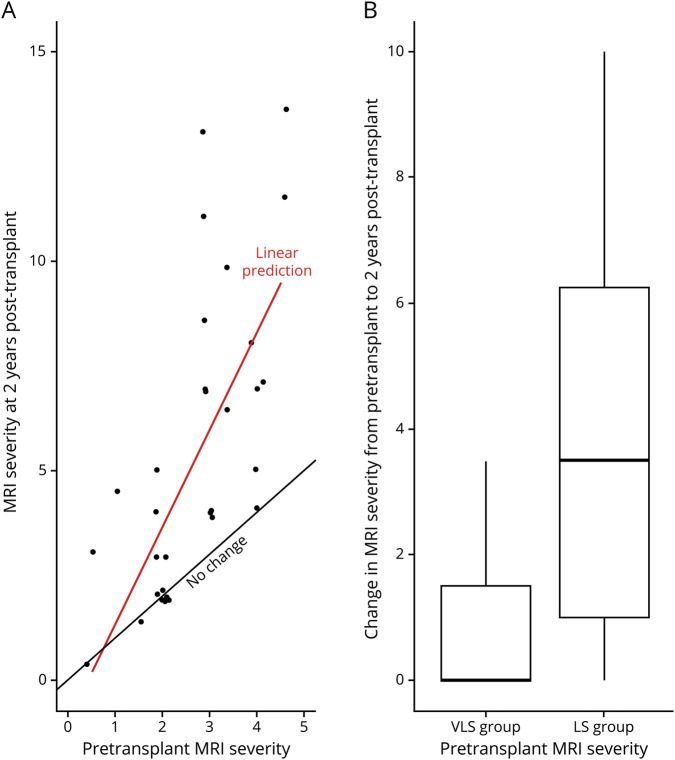
Patients whose pretransplant lesion extended beyond the splenium of the corpus callosum and adjacent periventricular white matter (MRI severity score >2) demonstrated lower posttransplant neurocognitive scores, more neuropsychiatric symptoms, and more disease progression on MRI than patients with a less severe lesion. Changes from baseline neurocognitive functioning were greater at 2 years posttransplant as compared to 1 year. There was greater variance and risk of lesion progression as pretransplant MRI severity increased.
To realize the full benefits of newborn screening, clinicians must detect very small demyelinating lesions during surveillance and intervene quickly. Novel interventions that reduce risks inherent in allogeneic transplantation are needed. Trial endpoints should include direct neurocognitive assessment and extend at least 2 years posttreatment to provide the greatest sensitivity to detect neurocognitive morbidity.
通过对 X 连锁肾上腺脑白质营养不良(ALD)进行新生儿筛查监测,量化可能实现的基准治疗结果。我们报告了在脱髓鞘的早期阶段,即疾病出现神经认知迹象之前,接受造血干细胞移植(HSCT)的男孩的神经认知、神经心理和 MRI 变化。
回顾性病历审查确定了 36 名患者,他们的脑 ALD 在早期被发现并得到治疗,其病变严重程度低于 ALD 特定的 MRI 评分系统的 5 分。移植时的中位年龄为 7.3 岁(范围,4.0-16.1 岁)。对 33 名患者的 2 年 HSCT 后 MRI 疾病进展与初始病变严重程度进行了比较,并对 30 名患者进行了纵向神经认知和神经心理结局研究。
与病变较轻的患者相比,移植前病变延伸至胼胝体体部的穹窿和邻近的脑室周围白质(MRI 严重程度评分>2)的患者在移植后具有较低的神经认知评分、更多的神经精神症状和更多的 MRI 疾病进展。与移植后 1 年相比,移植后 2 年的神经认知功能变化更大。随着移植前 MRI 严重程度的增加,变化的差异和病变进展的风险更大。
为了实现新生儿筛查的全部益处,临床医生必须在监测期间发现非常小的脱髓鞘病变,并迅速干预。需要新的干预措施来降低异基因移植固有的风险。试验终点应包括直接的神经认知评估,并至少延长至治疗后 2 年,以提供最大的敏感性来检测神经认知障碍。