Department of Respiratory, Allergy and Sleep Research, Akademiska Sjukhuset, Uppsala University, 751 85, Uppsala, Sweden.
Department of Respiratory Medicine and Allergology, Akademiska Sjukhuset, Uppsala, Sweden.
Sleep Breath. 2021 Jun;25(2):587-596. doi: 10.1007/s11325-020-02086-1. Epub 2020 Jul 6.
To study changes in lung function among individuals with a risk of obstructive sleep apnoea (OSA), and if asthma affected this relationship.
We used data from the European Community Respiratory Health Survey II and III, a multicentre general population study. Participants answered questionnaires and performed spirometry at baseline and 10-year follow-up (n = 4,329 attended both visits). Subjects with high risk for OSA were identified from the multivariable apnoea prediction (MAP) index, calculated from BMI, age, gender, and OSA symptoms at follow-up. Asthma was defined as having doctor's diagnosed asthma at follow-up. Primary outcomes were changes in forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) from baseline to follow-up.
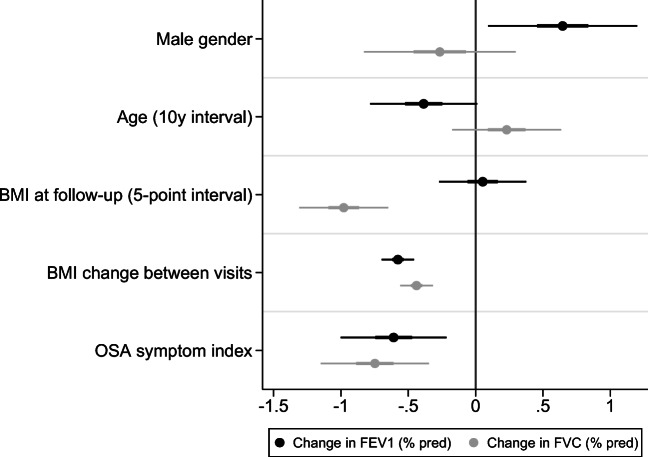
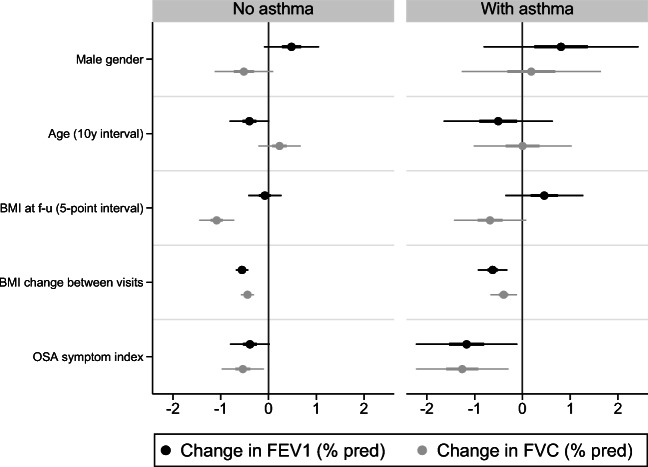
Among 5108 participants at follow-up, 991 (19%) had a high risk of OSA based on the MAP index. Participants with high OSA risk more often had wheeze, cough, chest tightness, and breathlessness at follow-up than those with low OSA risk. Lung function declined more rapidly in subjects with high OSA risk (low vs high OSA risk [mean ± SD]: FEV1 = - 41.3 ± 24.3 ml/year vs - 50.8 ± 30.1 ml/year; FVC = - 30.5 ± 31.2 ml/year vs - 45.2 ± 36.3 ml/year). Lung function decline was primarily associated with higher BMI and OSA symptoms. OSA symptoms had a stronger association with lung function decline among asthmatics, compared to non-asthmatics.
In the general population, a high probability of obstructive sleep apnoea was related to faster lung function decline in the previous decade. This was driven by a higher BMI and more OSA symptoms among these subjects. The association between OSA symptoms and lung function decline was stronger among asthmatics.
研究阻塞性睡眠呼吸暂停(OSA)高危人群的肺功能变化,以及哮喘是否影响这种关系。
我们使用了来自欧洲社区呼吸健康调查 II 和 III 的数据,这是一项多中心的一般人群研究。参与者在基线和 10 年随访时回答问卷并进行肺功能检查(n=4329 人参加了两次随访)。根据多变量呼吸暂停预测(MAP)指数,从 BMI、年龄、性别和随访时的 OSA 症状中确定 OSA 高危人群。哮喘定义为随访时被医生诊断为哮喘。主要结局是从基线到随访时用力呼气量 1 秒(FEV1)和用力肺活量(FVC)的变化。
在随访的 5108 名参与者中,根据 MAP 指数,有 991 人(19%)有 OSA 高危。与低 OSA 风险组相比,高 OSA 风险组在随访时更常出现喘息、咳嗽、胸闷和呼吸困难。高 OSA 风险组的肺功能下降速度更快(低 vs 高 OSA 风险[平均±标准差]:FEV1=-41.3±24.3ml/年 vs -50.8±30.1ml/年;FVC=-30.5±31.2ml/年 vs -45.2±36.3ml/年)。肺功能下降主要与更高的 BMI 和 OSA 症状有关。与非哮喘患者相比,哮喘患者的 OSA 症状与肺功能下降的相关性更强。
在一般人群中,阻塞性睡眠呼吸暂停的可能性较高与前十年肺功能下降较快有关。这是由于这些患者的 BMI 更高,OSA 症状更多。OSA 症状与肺功能下降之间的关联在哮喘患者中更强。