Delfau-Larue Marie-Helene, Boulland Marie-Laure, Beldi-Ferchiou Asma, Feugier Pierre, Maisonneuve Hervé, Casasnovas Rene-Olivier, Lemonnier François, Pica Gian Matteo, Houot Roch, Ysebaert Loic, Tilly Hervé, Eisenmann Jean-Claude, Le Gouill Steven, Ribrag Vincent, Godmer Pascal, Glaisner Sylvie, Cartron Guillaume, Xerri Luc, Salles Gilles André, Fest Thierry, Morschhauser Franck
Biological Hematology and Immunology Department, Groupe Hospitalier Mondor, INSERM U955, Creteil, France.
Hematobiology Department, Centre Hospitalo-Universitaire (CHU) Pontchaillou, Rennes, France.
Blood Adv. 2020 Aug 11;4(14):3217-3223. doi: 10.1182/bloodadvances.2020001955.
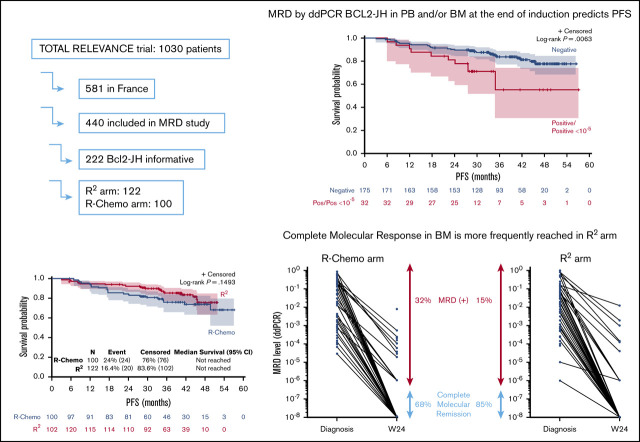
Complete molecular response (CMR) after first-line immunochemotherapy reflects treatment efficacy and may predict prognosis in patients with follicular lymphoma (FL). RELEVANCE is the first phase 3 trial comparing the chemotherapy-free regimen lenalidomide/rituximab (R2) vs rituximab/chemotherapy (R-Chemo) in previously untreated FL patients (ClinicalTrials.gov identifier: NCT01650701). The objective of the minimal residual disease (MRD) analysis was to determine the ability of a chemotherapy-free regimen to induce CMR. Of 440 French patients participating in the Lymphoma Study Association (LYSA) RELEVANCE MRD study, all 222 patients with a BIOMED-2-detectable BCL2-JH translocation at diagnosis were analyzed. MRD was quantified by droplet digital polymerase chain reaction with a sensitivity ≤10-4. At week 24 (end of induction treatment), 98% and 78% of patients achieved CMR in peripheral blood (PB) and bone marrow (BM), respectively. Achievement of CMR (in PB and/or BM) had a significant impact on progression-free survival (PFS), with 3-year PFS of 84% and 55% for patients with CMR and detectable MRD, respectively (P = .015). CMR at week 24 was reached more frequently in the R2 arm (105/117; 90%) than in the R-Chemo arm (70/90; 77%) (P = .022). The poor prognostic value in terms of PFS for the persistence of molecular disease was observed irrespective of treatment arm (interaction test, P = .31). In agreement with the clinical results of the RELEVANCE trial, our results show that R2 immunomodulatory treatment in first-line FL can achieve high rates of CMR.
一线免疫化疗后的完全分子缓解(CMR)反映了治疗效果,并可能预测滤泡性淋巴瘤(FL)患者的预后。RELEVANCE是第一项在初治FL患者中比较无化疗方案来那度胺/利妥昔单抗(R2)与利妥昔单抗/化疗(R-化疗)的3期试验(ClinicalTrials.gov标识符:NCT01650701)。微小残留病(MRD)分析的目的是确定无化疗方案诱导CMR的能力。在参与淋巴瘤研究协会(LYSA)RELEVANCE MRD研究的440例法国患者中,对所有222例诊断时可通过BIOMED-2检测到BCL2-JH易位的患者进行了分析。通过灵敏度≤10-4的液滴数字聚合酶链反应对MRD进行定量。在第24周(诱导治疗结束时),分别有98%和78%的患者在外周血(PB)和骨髓(BM)中实现了CMR。CMR(在PB和/或BM中)的实现对无进展生存期(PFS)有显著影响,CMR患者和可检测到MRD的患者3年PFS分别为84%和55%(P = 0.015)。在R2组(105/117;90%)中,第24周达到CMR的频率高于R-化疗组(70/90;77%)(P = 0.022)。无论治疗组如何,均观察到分子疾病持续存在对PFS的预后价值较差(交互检验,P = 0.31)。与RELEVANCE试验的临床结果一致,我们的结果表明,一线FL的R2免疫调节治疗可实现高比例的CMR。