Department of Epidemiology & Biostatistics, Amsterdam Public Health Research Institute, Amsterdam UMC - Location VU University Medical Center, Amsterdam, The Netherlands.
Department of Internal Medicine and Geriatrics, Amsterdam UMC - Location VU University Medical Center, Amsterdam, The Netherlands.
J Am Geriatr Soc. 2020 Nov;68(11):2587-2593. doi: 10.1111/jgs.16716. Epub 2020 Jul 23.
BACKGROUND/OBJECTIVES: Frailty, loneliness, and social isolation are all associated with adverse outcomes in older adults, but little is known about their combined impact on mortality.
Prospective cohort study.
The Longitudinal Aging Study Amsterdam.
Community-dwelling older adults aged 65 and older (n = 1,427).
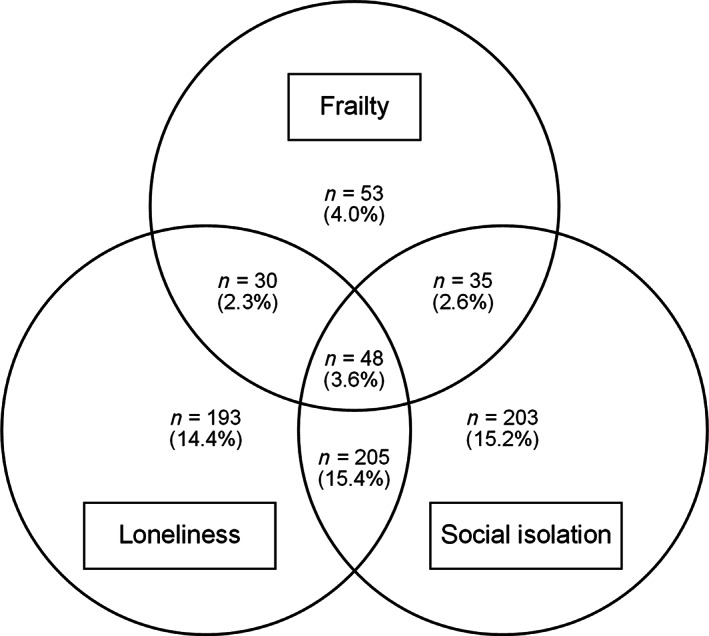
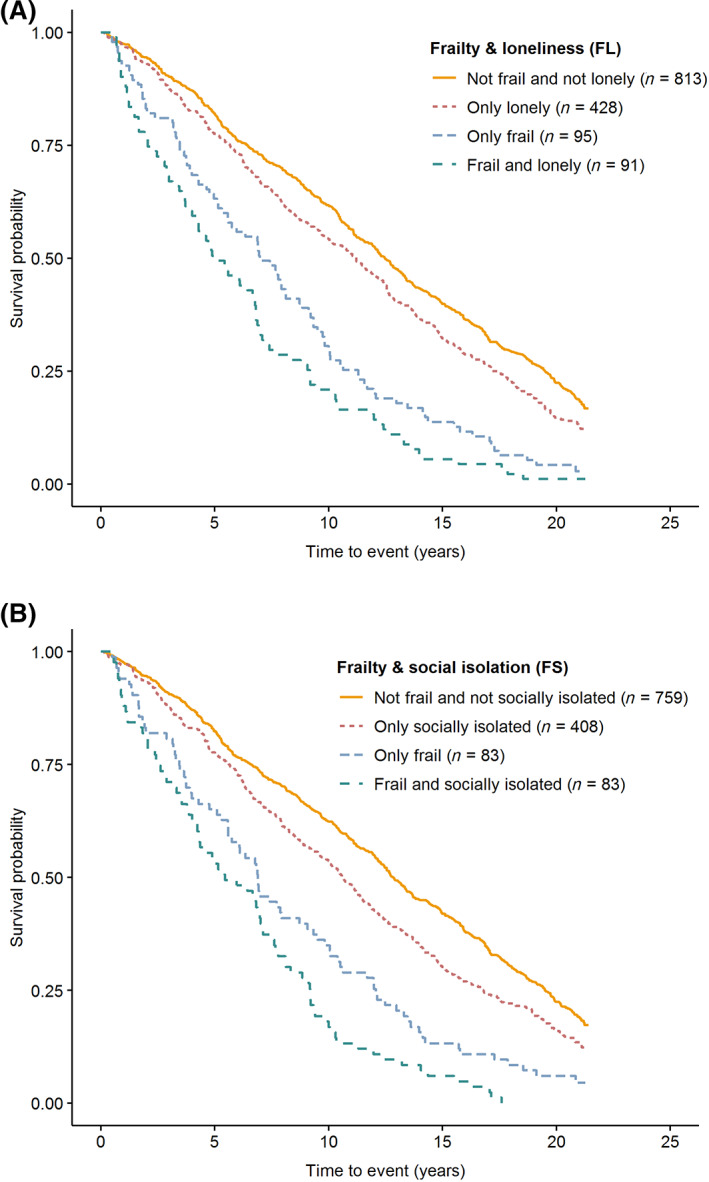
Frailty was measured with the frailty phenotype (Fried criteria). Loneliness was assessed with the De Jong Gierveld Loneliness Scale. Social isolation was operationalized using information on partner status, social support, and network size. Two categorical variables were created, for each possible combination regarding frailty and loneliness (FL) and frailty and social isolation (FS), respectively. Mortality was monitored over a period of 22 years (1995-2017). Survival curves and Cox proportional hazard models were used to study the effects of the FL and FS combinations on mortality. Analyses were adjusted for sociodemographic factors, depression, chronic diseases, and smoking.
Frailty prevalence was 13%, and 5.9% of the sample were frail and lonely, and 6.2% frail and socially isolated. In fully adjusted models, older adults who were only frail had a higher risk of mortality compared with people without any of the conditions (hazard ratio [HR] range = 1.40-1.48; P < .01). However, the highest risk of mortality was observed in people with a combined presence of frailty and loneliness or social isolation (HR = 1.83; 95% confidence interval [CI] = 1.42-2.37; HR = 1.77; 95% CI = 1.36-2.30). Sensitivity analyses using a frailty index based on the deficit accumulation approach instead of the frailty phenotype showed similar results, confirming the robustness of our findings.
Frail older adults are at increased risk of mortality, but this risk is even higher for those who are also lonely or socially isolated. To optimize well-being and health outcomes in physically frail older adults, targeted interventions focusing on both subjective and objective social vulnerability are needed.
背景/目的:衰弱、孤独和社会隔离都与老年人的不良结局有关,但人们对它们对死亡率的综合影响知之甚少。
前瞻性队列研究。
阿姆斯特丹纵向老龄化研究。
年龄在 65 岁及以上的社区居住的老年人(n=1427)。
衰弱用衰弱表型(Fried 标准)测量。孤独用 Jong Gierveld 孤独量表评估。社会隔离通过伴侣状况、社会支持和网络规模的信息来操作化。为每个可能的衰弱和孤独(FL)和衰弱和社会隔离(FS)组合创建了两个分类变量。在 22 年的时间内(1995-2017 年)监测死亡率。使用生存曲线和 Cox 比例风险模型研究 FL 和 FS 组合对死亡率的影响。分析调整了社会人口因素、抑郁、慢性疾病和吸烟。
衰弱的患病率为 13%,样本中有 5.9%的人衰弱且孤独,6.2%的人衰弱且社会隔离。在完全调整的模型中,与没有任何这些情况的人相比,只有衰弱的老年人死亡风险更高(风险比范围=1.40-1.48;P<.01)。然而,在同时存在衰弱和孤独或社会隔离的人群中,观察到最高的死亡风险(HR=1.83;95%置信区间[CI]=1.42-2.37;HR=1.77;95%CI=1.36-2.30)。使用基于缺陷积累方法的衰弱指数而不是衰弱表型的敏感性分析显示了类似的结果,证实了我们研究结果的稳健性。
衰弱的老年人死亡风险增加,但对于那些孤独或社会隔离的老年人来说,风险更高。为了优化身体虚弱的老年人的幸福感和健康结果,需要针对主观和客观社会脆弱性进行有针对性的干预。