Thoracic Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, New York.
Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center, New York, New York.
Semin Thorac Cardiovasc Surg. 2021;33(1):206-216. doi: 10.1053/j.semtcvs.2020.08.006. Epub 2020 Aug 25.
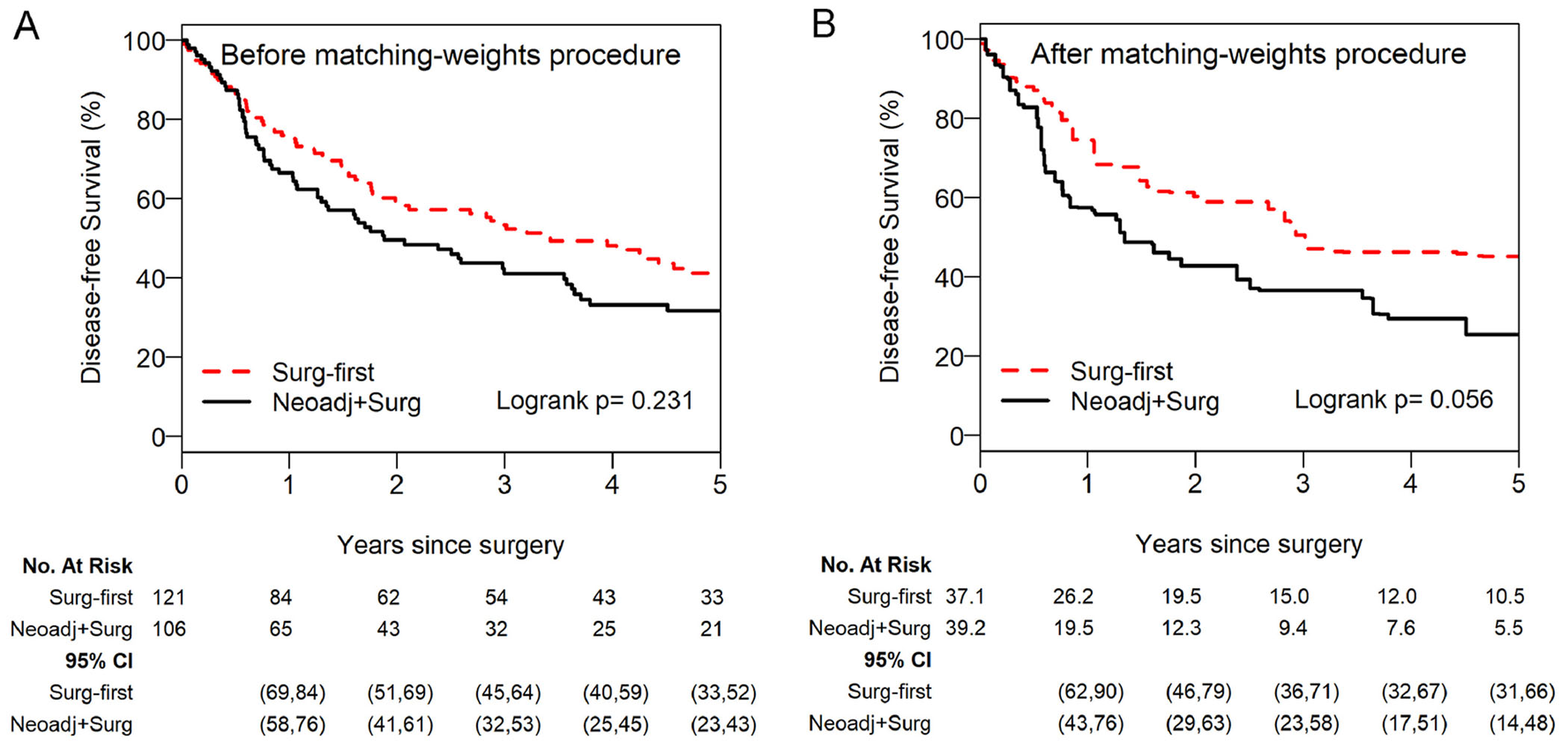
The optimal treatment strategy for pathologic single-station N2 (pN2a1) non-small cell lung cancer (NSCLC)-surgery first followed by adjuvant treatment (SF) or neoadjuvant therapy followed by surgery (NS)-remains unclear. We compared disease-free survival (DFS) and overall survival (OS) after NS versus SF for pN2a1 NSCLC. We retrospectively identified patients with pN2a1 NSCLC resected between 2000 and 2018. Patients in the SF group had cN0 disease and were treated with surgery before adjuvant chemotherapy; patients in the NS group had known preoperative nodal disease, cN2 disease, and were treated with neoadjuvant therapy before surgery. The matching-weights procedure was applied to generate a cohort with similar characteristics between groups. DFS and OS were calculated using the Kaplan-Meier approach and compared between groups using weighted log-rank test and Cox proportional hazards models. We identified 227 patients with pN2a1 disease: 121 treated with SF and 106 with NS. After the matching-weights procedure, 5- and 10-year DFS were 45% and 27% for SF versus 26% and 21% for NS (log-rank P = 0.056; hazard ratio [HR], 1.61; 95% confidence interval [CI], 0.98-2.65); 5- and 10-year OS were 49% and 30% for SF versus 43% and 20% for NS (log-rank P = 0.428; HR, 1.24; 95% CI, 0.67-2.28). SF and NS for pN2a1 NSCLC resulted in similar survival. A study comparing SF for known preresectional pN2a1 with occult pN2a1 disease could be a next step. Further investigation of SF for known N2a1 versus occult pN2a1 disease could power a clinical trial focused on N2a NSCLC.
对于病理单站 N2(pN2a1)非小细胞肺癌(NSCLC)-手术优先辅以治疗(SF)或新辅助治疗后手术(NS)的最佳治疗策略仍不清楚。我们比较了 NS 与 SF 治疗 pN2a1 NSCLC 的无病生存(DFS)和总生存(OS)。我们回顾性地确定了 2000 年至 2018 年间接受手术切除的 pN2a1 NSCLC 患者。SF 组的患者为 cN0 疾病,并在辅助化疗前接受手术治疗;NS 组的患者为术前已知的淋巴结疾病,cN2 疾病,并在手术前接受新辅助治疗。应用匹配权重程序在两组之间生成具有相似特征的队列。使用 Kaplan-Meier 方法计算 DFS 和 OS,并使用加权对数秩检验和 Cox 比例风险模型比较组间差异。我们确定了 227 例 pN2a1 疾病患者:121 例接受 SF 治疗,106 例接受 NS 治疗。在匹配权重程序后,SF 的 5 年和 10 年 DFS 分别为 45%和 27%,而 NS 分别为 26%和 21%(对数秩 P = 0.056;风险比 [HR],1.61;95%置信区间 [CI],0.98-2.65);SF 的 5 年和 10 年 OS 分别为 49%和 30%,而 NS 分别为 43%和 20%(对数秩 P = 0.428;HR,1.24;95% CI,0.67-2.28)。SF 和 NS 治疗 pN2a1 NSCLC 的生存结果相似。下一步可以进行一项比较术前已知 pN2a1 与隐匿性 pN2a1 疾病的 SF 的研究。进一步研究 SF 治疗已知 N2a1 与隐匿性 pN2a1 疾病的差异可能会为一项专注于 N2a NSCLC 的临床试验提供动力。