Department of Pulmonary and Critical Care Medicine, National Clinical Research Center for Respiratory Diseases, Institute of Respiratory Medicine, Chinese Academy of Medical Sciences, China-Japan Friendship Hospital, No 2, East Yinghua Road, Chaoyang District, Beijing, 100029, China.
School of Biological Science and Medical Engineering, Beihang University, Beijing, 100191, China.
BMC Infect Dis. 2020 Aug 27;20(1):637. doi: 10.1186/s12879-020-05360-5.
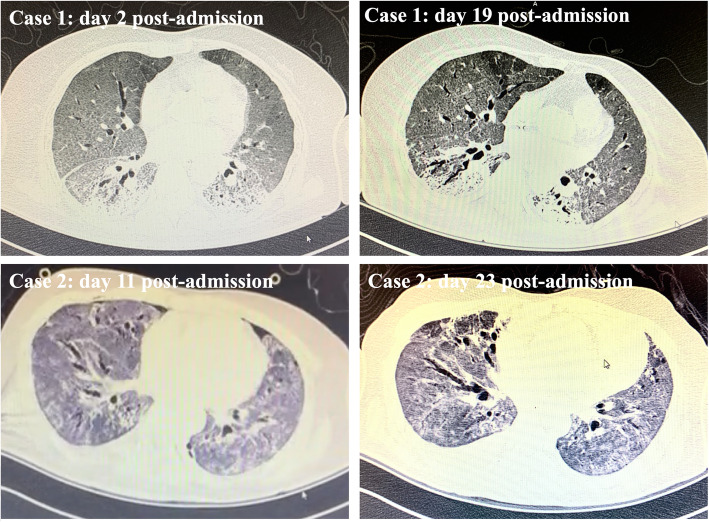
An ongoing outbreak of coronavirus disease 2019 (COVID-19) is spreading globally. Recently, several articles have mentioned that the early acute respiratory distress syndrome (ARDS) caused by COVID-19 significantly differ from those of ARDS due to other causes. Actually, we newly observed that some mechanically ventilated COVID-19 patients recovering from severe ARDS (more than 14 days after invasive ventilation) often experienced evidently gradual increases in CO retention and minute ventilation. However, the underlying mechanics remain unclear.
To explain these pathophysiological features and discuss the ventilatory strategy during the late phase of severe ARDS in COVID-19 patients, we first used a metabolic module on a General Electric R860 ventilator (Engstrom Carestation; GE Healthcare, USA) to monitor parameters related to gas metabolism, lung mechanics and physiological dead space in two COVID-19 patients. We found that remarkably decreased ventilatory efficiency (e.g., the ratio of dead space to tidal volume 70-80%, arterial to end-tidal CO difference 18-23 mmHg and ventilatory ratio 3-4) and hypermetabolism (oxygen consumption 300-400 ml/min, CO elimination 200-300 ml/min) may explain why these patients experienced more severe respiratory distress and CO retention in the late phase of ARDS caused by COVID-19.
During the recovery period of ARDS among mechanically-ventilated COVID-19 patients, attention should be paid to the monitoring of physiological dead space and metabolism. Tidal volume (8-9 ml/kg) could be increased appropriately under the limited plateau pressure; however, barotrauma should still be kept in mind.
目前,新型冠状病毒病 2019(COVID-19)的爆发正在全球范围内蔓延。最近,有几篇文章提到,COVID-19 早期引起的急性呼吸窘迫综合征(ARDS)与其他病因引起的 ARDS 明显不同。实际上,我们最近观察到,一些接受机械通气的 COVID-19 患者在重度 ARDS (经有创通气 14 天后)康复过程中,常常出现二氧化碳潴留和分钟通气量逐渐增加的现象。然而,其潜在的发病机制尚不清楚。
为了解释这些病理生理学特征,并讨论 COVID-19 患者重度 ARDS 后期的通气策略,我们首先使用通用电气 R860 呼吸机(美国通用电气医疗保健公司的 Engstrom Carestation)上的代谢模块,监测了 2 例 COVID-19 患者与气体代谢、肺力学和生理死腔相关的参数。我们发现,通气效率显著降低(例如,死腔与潮气量的比值为 70-80%,动脉与呼气末二氧化碳的差值为 18-23mmHg,通气比为 3-4)和高代谢(氧耗 300-400ml/min,CO 清除 200-300ml/min)可能解释了为什么这些患者在 COVID-19 引起的 ARDS 晚期会出现更严重的呼吸困难和二氧化碳潴留。
在接受机械通气的 COVID-19 患者 ARDS 恢复期,应注意监测生理死腔和代谢情况。在限制平台压的情况下,可以适当增加潮气量(8-9ml/kg),但仍需注意气压伤。