Subbiah Vivek, Gervais Radj, Riely Gregory, Hollebecque Antoine, Blay Jean-Yves, Felip Enriqueta, Schuler Martin, Gonçalves Anthony, Italiano Antonio, Keedy Vicki, Chau Ian, Puzanov Igor, Raje Noopur S, Meric-Bernstam Funda, Makrutzki Martina, Riehl Todd, Pitcher Bethany, Baselga Jose, Hyman David M
University of Texas MD Anderson Cancer Center, Houston, TX.
Centre François Baclesse, Caen, France.
JCO Precis Oncol. 2019 Jun 27;3. doi: 10.1200/PO.18.00266. eCollection 2019.
To study whether V600 mutations in non-small-cell lung cancer (NSCLC) may indicate sensitivity to the BRAF inhibitor vemurafenib, we included a cohort of patients with NSCLC in the vemurafenib basket (VE-BASKET) study. On the basis of observed early clinical activity, we expanded the cohort of patients with NSCLC. We present results from this cohort.
This open-label, histology-independent, phase II study included six prespecified cohorts, including patients with NSCLC, and a seventh all-comers cohort. Patients received vemurafenib (960 mg two times per day) until disease progression or unacceptable toxicity. The primary end point of the final analysis was objective response rate (Response Evaluation Criteria in Solid Tumors, version 1.1). Secondary end points included progression-free survival, overall survival, and safety. Because the prespecified clinical benefit endpoint was met in the initial NSCLC cohort, the cohort was expanded.
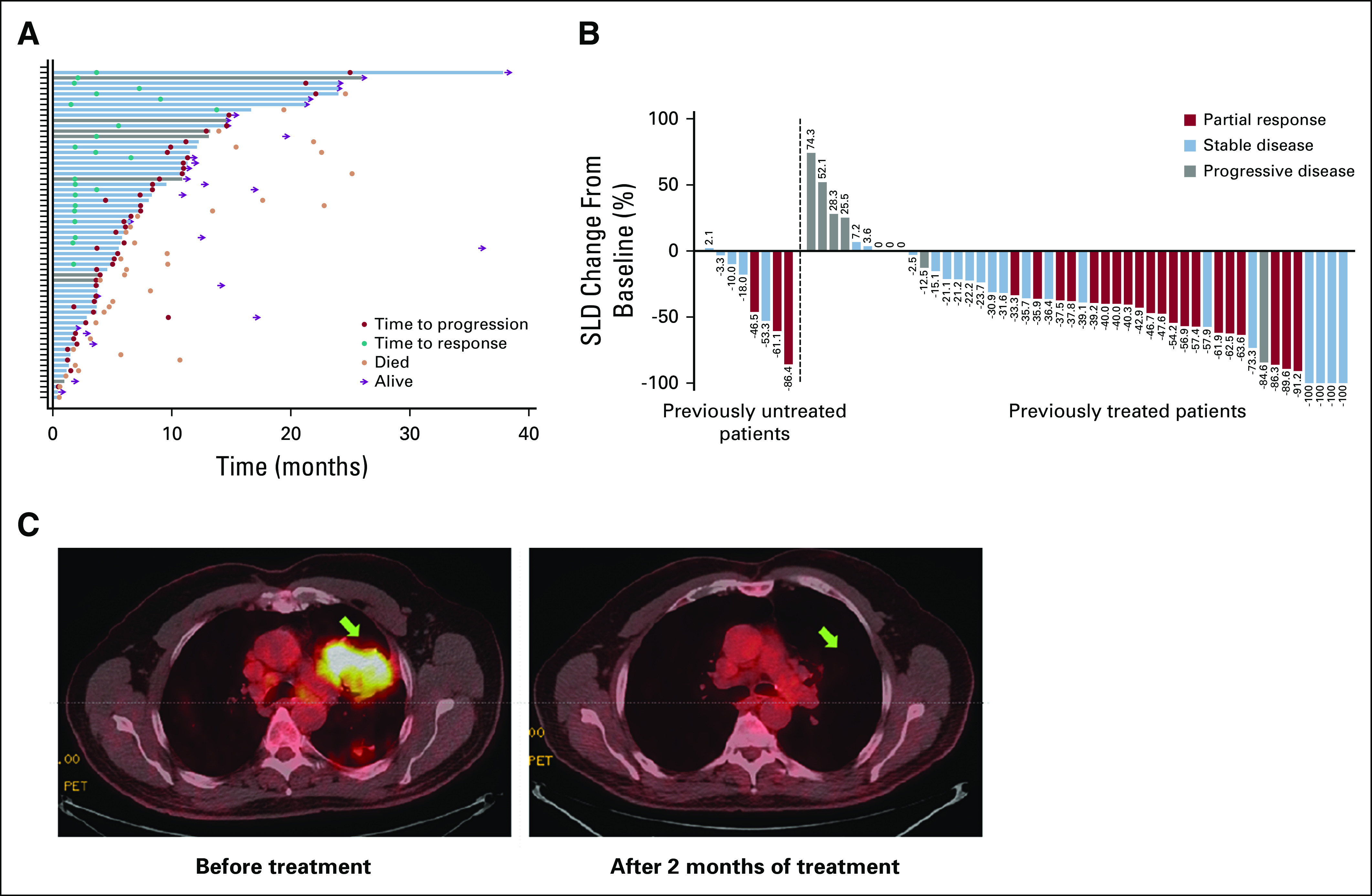
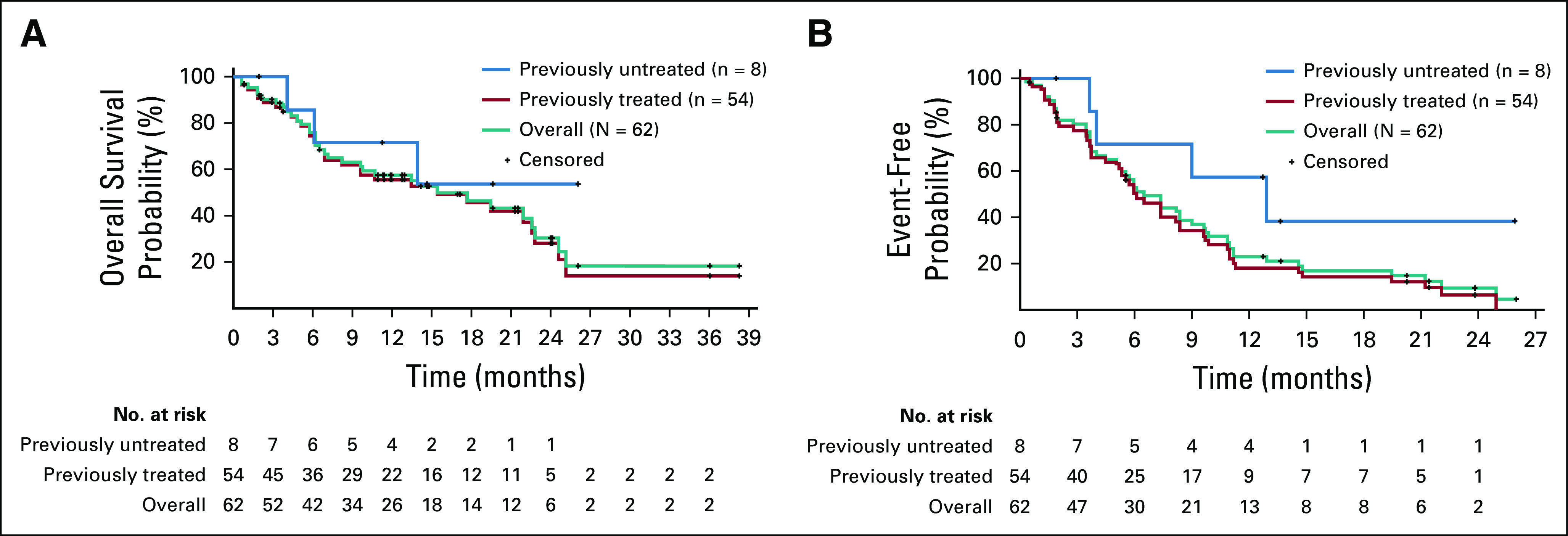
Sixty-two patients with V600-mutant NSCLC were enrolled and treated: 13% (n = 8) had received no prior systemic therapy, and 87% (n = 54) had received prior therapies. The objective response rate was 37.1% (95% CI, 25.2% to 50.3%) overall, 37.5% (95% CI, 8.5% to 75.5%) in previously untreated patients, and 37.0% (24.3% to 51.3%) in previously treated patients. Median progression-free survival was 6.5 months (95% CI, 5.2 to 9.0 months), and median overall survival was 15.4 months (95% CI, 9.6 to 22.8 months). The most common all-grade adverse event was nausea (40%). The safety profile of vemurafenib was similar to that observed in melanoma studies.
Vemurafenib showed promising activity in patients with NSCLC harboring V600 mutations. The safety profile of vemurafenib was similar to previous observations in patients with melanoma. Our results suggest a role for single-agent BRAF inhibition in patients with NSCLC and V600 mutations.
为了研究非小细胞肺癌(NSCLC)中的V600突变是否可能表明对BRAF抑制剂维莫非尼敏感,我们将一组NSCLC患者纳入维莫非尼篮子试验(VE-BASKET)研究。基于观察到的早期临床活性,我们扩大了NSCLC患者队列。我们展示了该队列的研究结果。
这项开放标签、不依赖组织学的II期研究包括六个预先指定的队列,其中包括NSCLC患者,以及第七个所有患者队列。患者接受维莫非尼(每日两次,每次960 mg)治疗,直至疾病进展或出现不可接受的毒性。最终分析的主要终点是客观缓解率(实体瘤疗效评价标准,第1.1版)。次要终点包括无进展生存期、总生存期和安全性。由于在最初的NSCLC队列中达到了预先指定的临床获益终点,因此该队列被扩大。
62例携带V600突变的NSCLC患者入组并接受治疗:13%(n = 8)未接受过先前的全身治疗,87%(n = 54)接受过先前的治疗。总体客观缓解率为37.1%(95%CI,25.2%至50.3%),既往未治疗患者为37.5%(95%CI,8.5%至75.5%),既往接受过治疗的患者为37.0%(24.3%至51.3%)。中位无进展生存期为6.5个月(95%CI,5.2至9.0个月),中位总生存期为15.4个月(95%CI,9.6至22.8个月)。最常见的所有级别的不良事件是恶心(40%)。维莫非尼的安全性与黑色素瘤研究中观察到的相似。
维莫非尼在携带V600突变的NSCLC患者中显示出有前景的活性。维莫非尼的安全性与先前在黑色素瘤患者中的观察结果相似。我们的结果表明单药BRAF抑制在携带V600突变的NSCLC患者中具有一定作用。