Department of Hospital Pharmacy, Erasmus University Medical Center, P.O. Box 2040, 3000 CA, Rotterdam, the Netherlands.
Department of Intensive Care, Maasstad Hospital, Rotterdam, The Netherlands.
Crit Care. 2020 Sep 15;24(1):558. doi: 10.1186/s13054-020-03272-z.
Early and appropriate antibiotic dosing is associated with improved clinical outcomes in critically ill patients, yet target attainment remains a challenge. Traditional antibiotic dosing is not suitable in critically ill patients, since these patients undergo physiological alterations that strongly affect antibiotic exposure. For beta-lactam antibiotics, the unbound plasma concentrations above at least one to four times the minimal inhibitory concentration (MIC) for 100% of the dosing interval (100%ƒT > 1-4×MIC) have been proposed as pharmacodynamic targets (PDTs) to maximize bacteriological and clinical responses. The objectives of this study are to describe the PDT attainment in critically ill patients and to identify risk factors for target non-attainment.
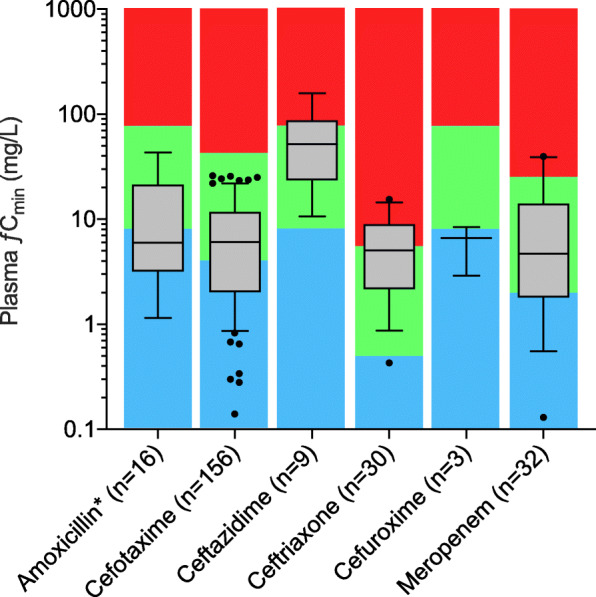
This prospective observational study was performed in two ICUs in the Netherlands. We enrolled adult patients treated with the following beta-lactam antibiotics: amoxicillin (with or without clavulanic acid), cefotaxime, ceftazidime, ceftriaxone, cefuroxime, and meropenem. Based on five samples within a dosing interval at day 2 of therapy, the time unbound concentrations above the epidemiological cut-off (ƒT > MIC and ƒT > 4×MIC) were determined. Secondary endpoints were estimated multivariate binomial and binary logistic regression models, for examining the association of PDT attainment with patient characteristics and clinical outcomes.
A total of 147 patients were included, of whom 63.3% achieved PDT of 100%ƒT > MIC and 36.7% achieved 100%ƒT > 4×MIC. Regression analysis identified male gender, estimated glomerular filtration rate (eGFR) ≥ 90 mL/min/1.73 m, and high body mass index (BMI) as risk factors for target non-attainment. Use of continuous renal replacement therapy (CRRT) and high serum urea significantly increased the probability of target attainment. In addition, we found a significant association between the 100%ƒT > MIC target attainment and ICU length of stay (LOS), but no significant correlation was found for the 30-day survival.
Traditional beta-lactam dosing results in low target attainment in the majority of critically ill patients. Male gender, high BMI, and high eGFR were significant risk factors for target non-attainment. These predictors, together with therapeutic drug monitoring, may help ICU clinicians in optimizing beta-lactam dosing in critically ill patients.
Netherlands Trial Registry (EXPAT trial), NTR 5632 . Registered on 7 December 2015.
在危重症患者中,早期和适当的抗生素剂量与改善临床结局相关,但目标达标仍然是一个挑战。传统的抗生素剂量不适合危重症患者,因为这些患者会经历强烈影响抗生素暴露的生理改变。对于β-内酰胺类抗生素,建议在 100%的给药间隔内(100%ƒT>1-4×MIC),至少有一次到四次高于最低抑菌浓度(MIC)的游离血浆浓度作为药效学目标(PDT),以最大限度地提高细菌学和临床反应。本研究的目的是描述危重症患者的 PDT 达标情况,并确定未达标目标的危险因素。
这是一项在荷兰的两个 ICU 进行的前瞻性观察研究。我们招募了接受以下β-内酰胺类抗生素治疗的成年患者:阿莫西林(有或无克拉维酸)、头孢噻肟、头孢他啶、头孢曲松、头孢呋辛和美罗培南。在治疗第 2 天的 5 个样本内,测定游离浓度超过流行病学切点(ƒT> MIC 和ƒT>4×MIC)的时间。次要终点是估计多变量二项式和二元逻辑回归模型,以检查 PDT 达标与患者特征和临床结局的关联。
共纳入 147 例患者,其中 63.3%达到 100%ƒT> MIC,36.7%达到 100%ƒT>4×MIC。回归分析确定男性、肾小球滤过率(eGFR)≥90ml/min/1.73m2和高体重指数(BMI)是未达标目标的危险因素。连续肾脏替代治疗(CRRT)和高血清尿素显著增加了达标概率。此外,我们发现 100%ƒT> MIC 目标达标与 ICU 住院时间(LOS)之间存在显著关联,但与 30 天生存率无显著相关性。
传统的β-内酰胺类药物剂量在大多数危重症患者中导致目标达标率较低。男性、高 BMI 和高 eGFR 是未达标目标的显著危险因素。这些预测因素,加上治疗药物监测,可能有助于 ICU 临床医生优化危重症患者的β-内酰胺类药物剂量。
荷兰试验注册处(EX-PAT 试验),NTR5632。于 2015 年 12 月 7 日注册。