Clinical Pharmacology, Janssen Research & Development LLC, San Diego, CA, USA.
Clinical Research Oncology, Janssen Research & Development LLC, Beerse, Belgium.
Pharmacol Res Perspect. 2020 Oct;8(5):e00649. doi: 10.1002/prp2.649.
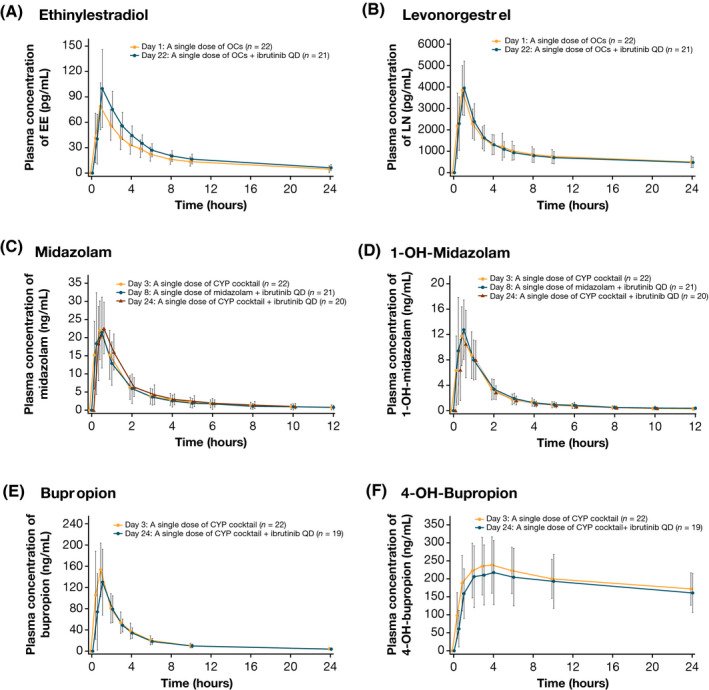
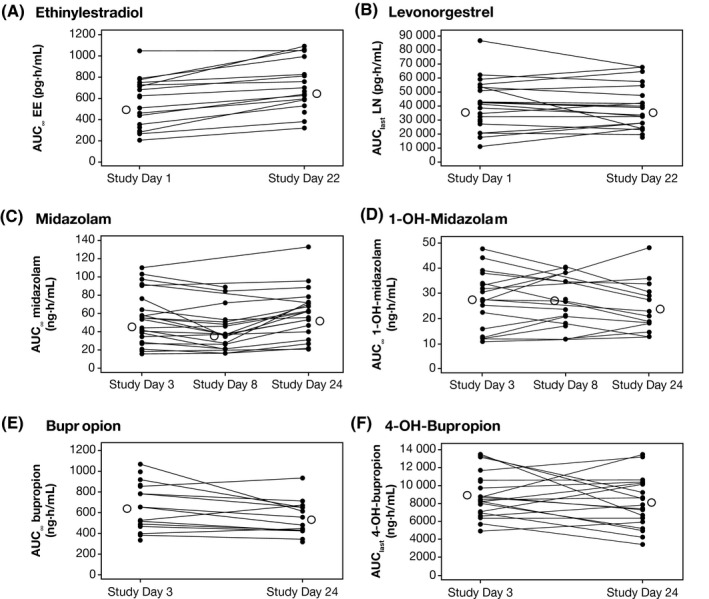
Ibrutinib may inhibit intestinal CYP3A4 and induce CYP2B6 and/or CYP3A. Secondary to potential induction, ibrutinib may reduce the exposure and effectiveness of oral contraceptives (OCs). This phase I study evaluated the effect of ibrutinib on the pharmacokinetics of the CYP2B6 substrate bupropion, CYP3A substrate midazolam, and OCs ethinylestradiol (EE) and levonorgestrel (LN). Female patients (N = 22) with B-cell malignancies received single doses of EE/LN (30/150 μg) and bupropion/midazolam (75/2 mg) during a pretreatment phase on days 1 and 3, respectively (before starting ibrutinib on day 8), and again after ibrutinib 560 mg/day for ≥ 2 weeks. Intestinal CYP3A inhibition was assessed on day 8 (single-dose ibrutinib plus single-dose midazolam). Systemic induction was assessed at steady-state on days 22 (EE/LN plus ibrutinib) and 24 (bupropion/midazolam plus ibrutinib). The geometric mean ratios (GMRs; test/reference) for maximum plasma concentration (C ) and area under the plasma concentration-time curve (AUC) were derived using linear mixed-effects models (90% confidence interval within 80%-125% indicated no interaction). On day 8, the GMR for midazolam exposure with ibrutinib coadministration was ≤ 20% lower than the reference, indicating lack of intestinal CYP3A4 inhibition. At ibrutinib steady-state, the C and AUC of EE were 33% higher than the reference, which was not considered clinically relevant. No substantial changes were noted for LN, midazolam, or bupropion. No unexpected safety findings were observed. A single dose of ibrutinib did not inhibit intestinal CYP3A4, and repeated administration did not induce CYP3A4/2B6, as assessed using EE, LN, midazolam, and bupropion.
依鲁替尼可能会抑制肠道 CYP3A4 并诱导 CYP2B6 和/或 CYP3A。由于潜在的诱导作用,依鲁替尼可能会降低口服避孕药(OC)的暴露和有效性。这项 I 期研究评估了依鲁替尼对 CYP2B6 底物丁丙诺啡、CYP3A 底物咪达唑仑和 OC 炔雌醇(EE)和左炔诺孕酮(LN)药代动力学的影响。患有 B 细胞恶性肿瘤的女性患者(N=22)在第 1 天和第 3 天分别接受 EE/LN(30/150μg)和丁丙诺啡/咪达唑仑(75/2mg)的单剂量治疗(在第 8 天开始依鲁替尼之前),并且在依鲁替尼 560mg/天后再次接受治疗至少 2 周。在第 8 天(依鲁替尼单剂量加咪达唑仑单剂量)评估肠道 CYP3A 抑制作用。在第 22 天(EE/LN 加依鲁替尼)和第 24 天(丁丙诺啡/咪达唑仑加依鲁替尼)评估稳态下的全身诱导作用。使用线性混合效应模型得出最大血浆浓度(C)和血浆浓度-时间曲线下面积(AUC)的几何均数比值(GMR;测试/参考)(90%置信区间在 80%-125%内表明无相互作用)。第 8 天,依鲁替尼联合给药时咪达唑仑暴露的 GMR 比参考值低≤20%,表明肠道 CYP3A4 抑制作用缺失。在依鲁替尼稳态时,EE 的 C 和 AUC 比参考值高 33%,但这并不被认为具有临床相关性。LN、咪达唑仑或丁丙诺啡没有明显变化。未观察到意外的安全性发现。单次给予依鲁替尼不会抑制肠道 CYP3A4,并且重复给药不会诱导 CYP3A4/2B6,这可通过 EE、LN、咪达唑仑和丁丙诺啡来评估。