Wu Shang-Gin, Chiang Chi-Lu, Liu Chien-Ying, Wang Chin-Chou, Su Po-Lan, Hsia Te-Chun, Shih Jin-Yuan, Chang Gee-Chen
Department of Internal Medicine, National Taiwan University Hospital, National Taiwan University, Taipei, Taiwan.
Department of Internal Medicine, National Taiwan University Cancer Center, National Taiwan University, Taipei, Taiwan.
Front Oncol. 2020 Sep 4;10:1481. doi: 10.3389/fonc.2020.01481. eCollection 2020.
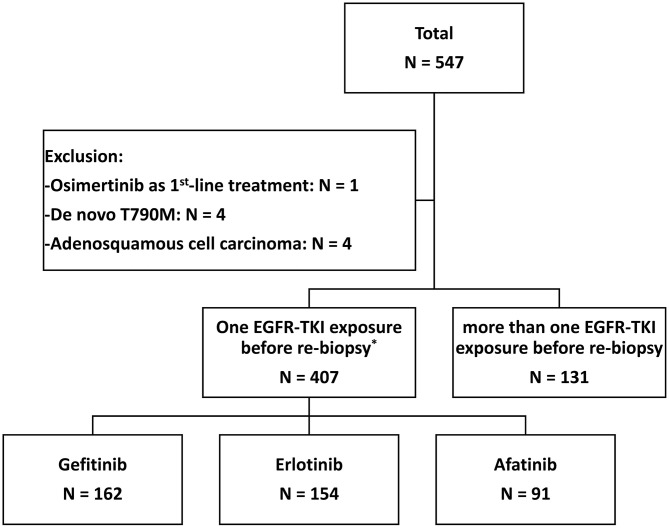
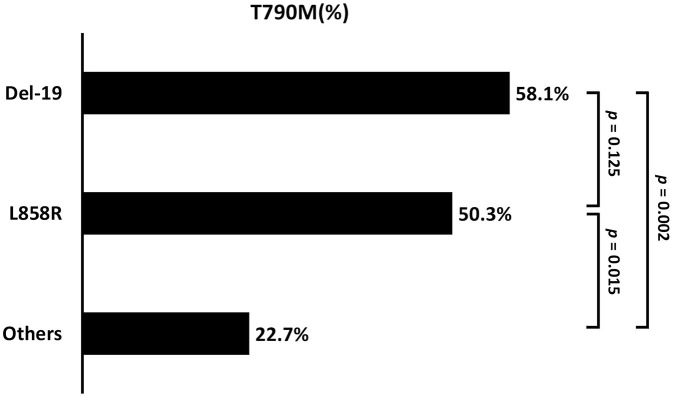
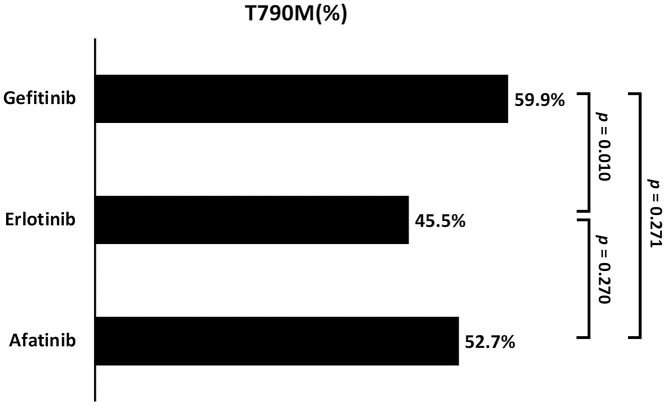
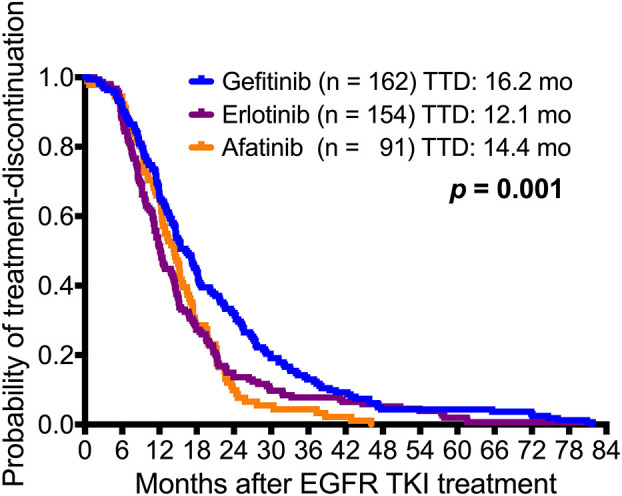
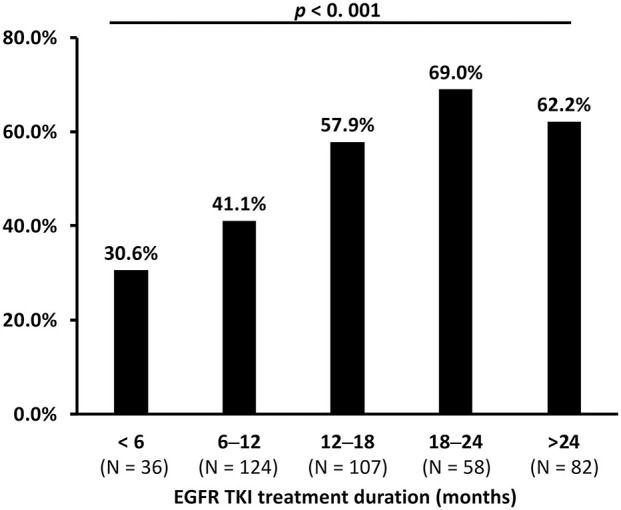
In Taiwan, epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (EGFR-TKIs), gefitinib, erlotinib, and afatinib are served as first-line therapy for non-small lung cell cancer (NSCLC) patients with sensitizing mutations. However, the majority of patients who initially respond to EGFR-TKIs, progress through acquiring T790M mutations (T790M), which is the most common resistant mechanism. Patients with T790M gain the opportunity of subsequent treatment with third-generation EGFR-TKI, osimertinib. This study aimed to evaluate the association between prior EGFR-TKI therapy and incidence of acquired T790M resistance in lung adenocarcinoma patients who have progressed on first/second-generation EGFR-TKI therapy. This retrospective study included lung adenocarcinoma patients who had a radiographically-confirmed progressive disease under EGFR-TKI treatment and had re-biopsy samples for T790M testing from seven medical centers in Taiwan from June 2013 to December 2018. Patients harboring T790M or using more than one EGFR-TKI were excluded. Of the 407 patients enrolled, the overall T790M acquisition rate was 52.8%. The patients treated with gefitinib, erlotinib or afatinib had a statistically significant difference in the T790M rates (59.9, 45.5, and 52.7%, respectively; = 0.037) after disease progression. Patients with common baseline mutations (Del-19 and L858R) ( = 0.005) and longer treatment duration with EGFR-TKIs ( < 0.001) had higher chances of T790M acquisition. Multivariate logistic regression analysis further showed that patients with common baseline mutations, gefitinib (compared to erlotinib) administration, and longer treatment duration with EGFR-TKIs had higher T790M incidence. There was no significant difference in the incidence of acquired T790M between different re-biopsy tissue samples or complications. In conclusion, this study showed that patients who progressed from gefitinib treatment, bearing common mutations, and with longer EGFR-TKI treatment duration had increased incidence of T790M acquisition and, therefore, were suitable for subsequent osimertinib treatment.
在台湾,表皮生长因子受体(EGFR)酪氨酸激酶抑制剂(EGFR-TKIs),吉非替尼、厄洛替尼和阿法替尼被用作具有敏感突变的非小细胞肺癌(NSCLC)患者的一线治疗。然而,大多数最初对EGFR-TKIs有反应的患者,会通过获得T790M突变(T790M)而进展,这是最常见的耐药机制。携带T790M的患者有机会接受第三代EGFR-TKI奥希替尼的后续治疗。本研究旨在评估在第一代/第二代EGFR-TKI治疗中进展的肺腺癌患者中,既往EGFR-TKI治疗与获得性T790M耐药发生率之间的关联。这项回顾性研究纳入了在2013年6月至2018年12月期间,来自台湾七个医疗中心的肺腺癌患者,这些患者在EGFR-TKI治疗下经影像学证实疾病进展,并进行了T790M检测的再次活检样本。排除携带T790M或使用过一种以上EGFR-TKI的患者。在纳入的407例患者中,总体T790M获得率为52.8%。在疾病进展后,接受吉非替尼、厄洛替尼或阿法替尼治疗的患者在T790M发生率上有统计学显著差异(分别为59.9%、45.5%和52.7%;P = 0.037)。具有常见基线突变(Del-19和L858R)(P = 0.005)以及EGFR-TKIs治疗持续时间较长(P < 0.001)的患者获得T790M的机会更高。多因素逻辑回归分析进一步显示,具有常见基线突变、接受吉非替尼(与厄洛替尼相比)治疗以及EGFR-TKIs治疗持续时间较长的患者T790M发生率更高。不同的再次活检组织样本或并发症之间获得性T790M的发生率没有显著差异。总之,本研究表明,从吉非替尼治疗进展而来、携带常见突变且EGFR-TKI治疗持续时间较长的患者T790M获得率增加,因此适合后续奥希替尼治疗。