Department of Medical Oncology, Tom Baker Cancer Center, 1331 29 ST NW, Calgary, Alberta, T2N 4N2, Canada.
University of Calgary, Calgary, Alberta, Canada.
BMC Cancer. 2020 Oct 15;20(1):1004. doi: 10.1186/s12885-020-07487-9.
Baseline cardiovascular disease (CVD) can impact the patterns of treatment and hence the outcomes of patients with lung cancer. This study aimed to characterize treatment trends and survival outcomes of patients with pre-existing CVD prior to their diagnosis of lung cancer.
We conducted a retrospective, population-based cohort study of patients with lung cancer diagnosed from 2004 to 2015 in a large Canadian province. Multivariable logistic regression and Cox regression models were constructed to determine the associations between CVD and treatment patterns, and its impact on overall (OS) and cancer-specific survival (CSS), respectively. A competing risk multistate model was developed to determine the excess mortality risk of patients with pre-existing CVD.
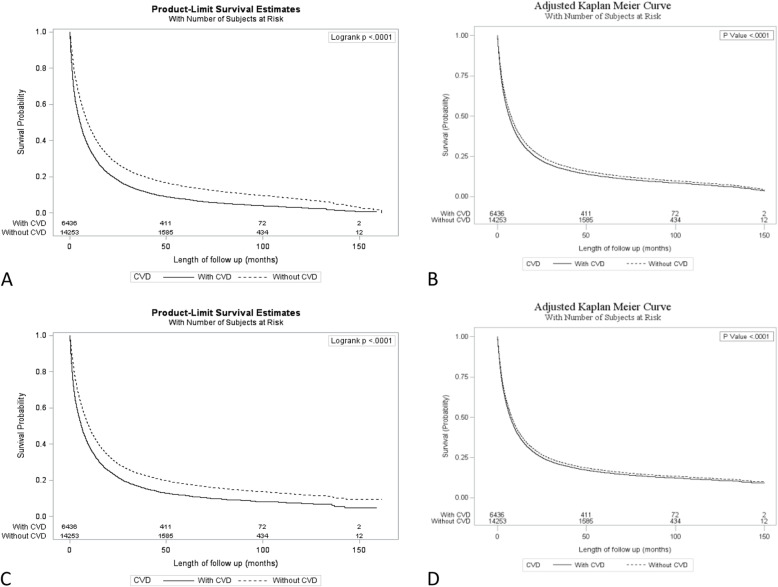
A total of 20,689 patients with lung cancer were eligible for the current analysis. Men comprised 55%, and the median age at diagnosis was 70 years. One-third had at least one CVD, with the most common being congestive heart failure in 15% of patients. Pre-existing CVD was associated with a lower likelihood of receiving chemotherapy (odds ratio [OR], 0.53; 95% confidence interval [CI], 0.48-0.58; P < .0001), radiotherapy (OR, 0.76; 95% CI, 0.7-0.82; P < .0001), and surgery (OR, 0.56; 95% CI, 0.44-0.7; P < .0001). Adjusting for measured confounders, the presence of pre-existing CVD predicted for inferior OS (hazard ratio [HR], 1.1; 95% CI, 1.1-1.2; P < .0001) and CSS (HR, 1.1; 95% CI, 1.1-1.1; P < .0001). However, in the competing risk multistate model that adjusted for baseline characteristics, prior CVD was associated with increased risk of non-cancer related death (HR, 1.48; 95% CI, 1.33-1.64; P < 0.0001) but not cancer related death (HR, 0.98; 95% CI, 0.94-1.03; P = 0.460).
Patients with lung cancer and pre-existing CVD are less likely to receive any modality of cancer treatment and are at a higher risk of non-cancer related deaths. As effective therapies such as immuno-oncology drugs are introduced, early cardio-oncology consultation may optimize management of lung cancer.
基线心血管疾病 (CVD) 可影响肺癌患者的治疗模式,进而影响其预后。本研究旨在分析肺癌患者在确诊前患有 CVD 的治疗趋势和生存结局。
我们开展了一项回顾性、基于人群的队列研究,纳入了 2004 年至 2015 年期间在加拿大一个大省确诊的肺癌患者。多变量逻辑回归和 Cox 回归模型用于确定 CVD 与治疗模式之间的关联,并分别评估其对总生存 (OS) 和癌症特异性生存 (CSS) 的影响。采用竞争风险多状态模型确定患有预先存在 CVD 的患者的超额死亡风险。
共纳入 20689 例肺癌患者,其中男性占 55%,中位诊断年龄为 70 岁。三分之一的患者至少患有一种 CVD,最常见的是心力衰竭(占 15%)。预先存在的 CVD 与接受化疗(比值比 [OR],0.53;95%置信区间 [CI],0.48-0.58;P<0.0001)、放疗(OR,0.76;95%CI,0.7-0.82;P<0.0001)和手术(OR,0.56;95%CI,0.44-0.7;P<0.0001)的可能性降低有关。在调整了测量混杂因素后,预先存在的 CVD 预示 OS 较差(风险比 [HR],1.1;95%CI,1.1-1.2;P<0.0001)和 CSS 较差(HR,1.1;95%CI,1.1-1.1;P<0.0001)。然而,在调整基线特征的竞争风险多状态模型中,预先存在的 CVD 与非癌症相关死亡的风险增加相关(HR,1.48;95%CI,1.33-1.64;P<0.0001),但与癌症相关死亡的风险无关(HR,0.98;95%CI,0.94-1.03;P=0.460)。
患有肺癌和预先存在 CVD 的患者接受任何癌症治疗方式的可能性较小,且非癌症相关死亡的风险较高。随着免疫肿瘤学药物等有效疗法的引入,早期心脏肿瘤学咨询可能会优化肺癌的管理。