Yu Jihion, Lim Bumjin, Lee Yongsoo, Park Jun-Young, Hong Bumsik, Hwang Jai-Hyun, Kim Young-Kug
Department of Anesthesiology and Pain Medicine.
Department of Urology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea.
Medicine (Baltimore). 2020 Oct 23;99(43):e22893. doi: 10.1097/MD.0000000000022893.
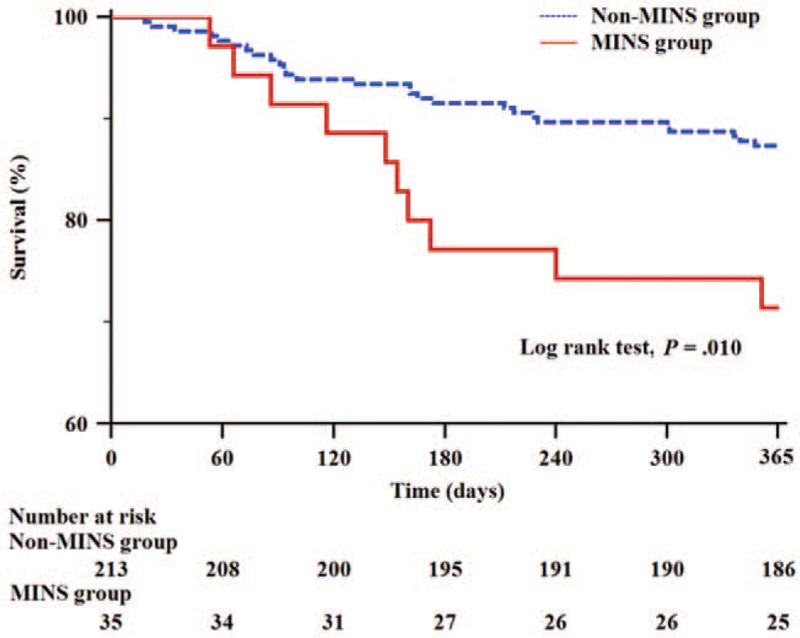
Radical cystectomy is considered the standard treatment for patients with muscle-invasive bladder tumors and has high postoperative complication rates among urological surgeries. High-risk patients, defined as those ≥45 years of age with history of coronary artery disease, stroke, or peripheral artery disease or those ≥65 years of age, can have a higher incidence of cardiac complications. Therefore, we evaluated the incidence, risk factors, and outcomes of myocardial injury after non-cardiac surgery (MINS) in high-risk patients who underwent radical cystectomy.This retrospective observational study analyzed 248 high-risk patients who underwent radical cystectomy. MINS was defined as serum troponin I concentration ≥0.04 mg/L within postoperative 3 days. The risk factors for MINS were evaluated by multivariate logistic regression analysis. Postoperative outcomes were evaluated. The 1-year survival after radical cystectomy was also compared between patients who developed MINS (MINS group) and those who did not (non-MINS group) by Kaplan-Meier analysis.MINS occurred in 35 patients (14.1%). Multivariate logistic regression analysis showed that early diastolic transmitral filling velocity (E)/early diastolic septal mitral annular velocity (E') ratio (odds ratio = 1.102, 95% confidence interval [1.009-1.203], P = .031) and large volume blood transfusion (odds ratio = 2.745, 95% confidence interval [1.131-6.664], P = .026) were significantly associated with MINS in high-risk patients who underwent radical cystectomy. Major adverse cardiac events and 1-year mortality were significantly higher in the MINS group than in the non-MINS group (17.1% vs 6.1%, P = .035; 28.6% vs 12.7%, P = .021, respectively). Kaplan-Meier analysis showed significantly lower 1-year survival in the MINS group than in the non-MINS group (P = .010).MINS occurred in 14.1% of patients. High E/E' ratio and large volume blood transfusion were risk factors for MINS in high-risk patients who underwent radical cystectomy. Postoperative major adverse cardiac events and 1-year mortality were significantly higher in the MINS group than in the non-MINS group. Preoperative evaluation of risk factors for MINS may provide useful information to detect cardiovascular complications after radical cystectomy in high-risk patients.
根治性膀胱切除术被认为是肌层浸润性膀胱肿瘤患者的标准治疗方法,在泌尿外科手术中术后并发症发生率较高。高危患者定义为年龄≥45岁且有冠状动脉疾病、中风或外周动脉疾病史的患者或年龄≥65岁的患者,其心脏并发症发生率可能更高。因此,我们评估了接受根治性膀胱切除术的高危患者非心脏手术后心肌损伤(MINS)的发生率、危险因素及预后。
这项回顾性观察性研究分析了248例接受根治性膀胱切除术的高危患者。MINS定义为术后3天内血清肌钙蛋白I浓度≥0.04mg/L。通过多因素逻辑回归分析评估MINS的危险因素。评估术后结局。采用Kaplan-Meier分析比较发生MINS的患者(MINS组)和未发生MINS的患者(非MINS组)根治性膀胱切除术后的1年生存率。
35例患者(14.1%)发生MINS。多因素逻辑回归分析显示,舒张早期二尖瓣血流速度(E)/舒张早期二尖瓣环间隔速度(E')比值(比值比=1.102,95%置信区间[1.009-1.203],P=0.031)和大量输血(比值比=2.745,95%置信区间[1.131-6.664],P=0.026)与接受根治性膀胱切除术的高危患者发生MINS显著相关。MINS组的主要不良心脏事件和1年死亡率显著高于非MINS组(分别为17.1%对6.1%,P=0.035;28.6%对12.7%,P=0.021)。Kaplan-Meier分析显示,MINS组的1年生存率显著低于非MINS组(P=0.010)。
14.1%的患者发生MINS。高E/E'比值和大量输血是接受根治性膀胱切除术的高危患者发生MINS的危险因素。MINS组术后主要不良心脏事件和1年死亡率显著高于非MINS组。术前评估MINS的危险因素可能为检测高危患者根治性膀胱切除术后的心血管并发症提供有用信息。