Division of Gastroenterology, Department of Medicine, University of California San Diego, La Jolla, California.
Division of Gastroenterology, University of Calgary, Calgary, Alberta, Canada.
Clin Gastroenterol Hepatol. 2021 Oct;19(10):2031-2045.e11. doi: 10.1016/j.cgh.2020.10.039. Epub 2020 Oct 27.
BACKGROUND & AIMS: We conducted a systematic review with meta-analysis to estimate rates and trends of colectomy in patients with ulcerative colitis (UC), and of primary and re-resection in patients with Crohn's disease (CD), focusing on contemporary risks.
Through a systematic review until September 3, 2019, we identified population-based cohort studies that reported patient-level cumulative risk of surgery in patients with UC and CD. We evaluated overall and contemporary risk (after 2000) of surgery and analyzed time trends through mixed-effects meta-regression.
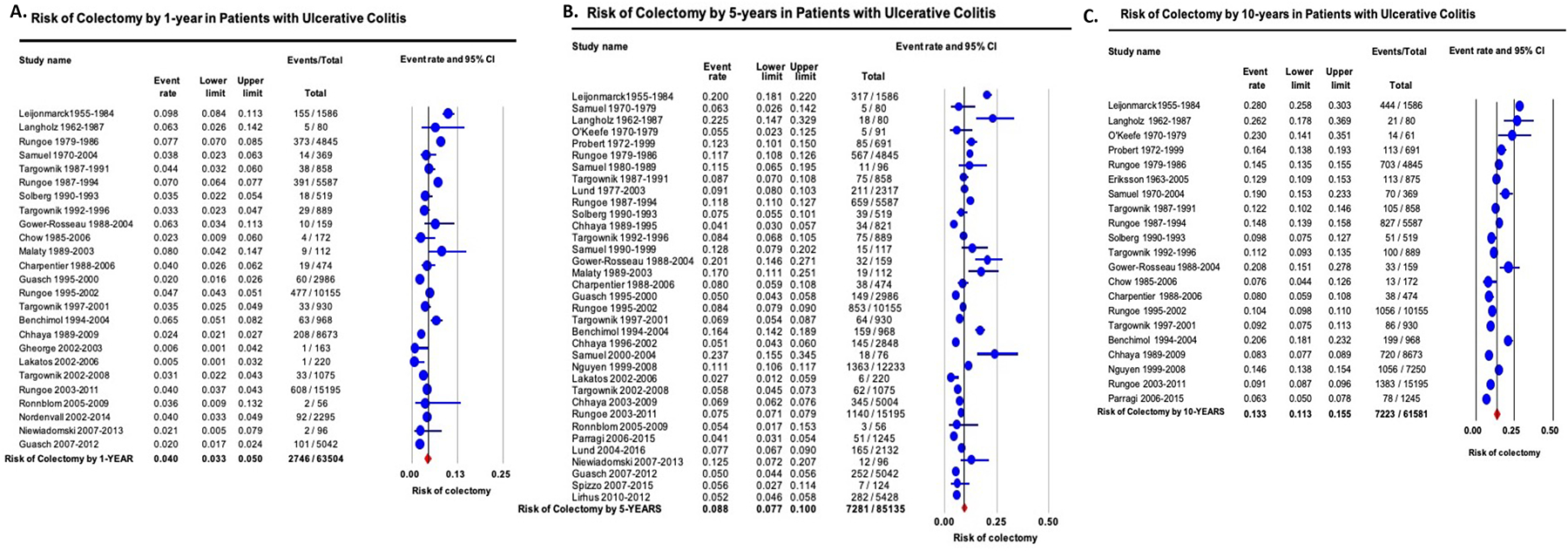
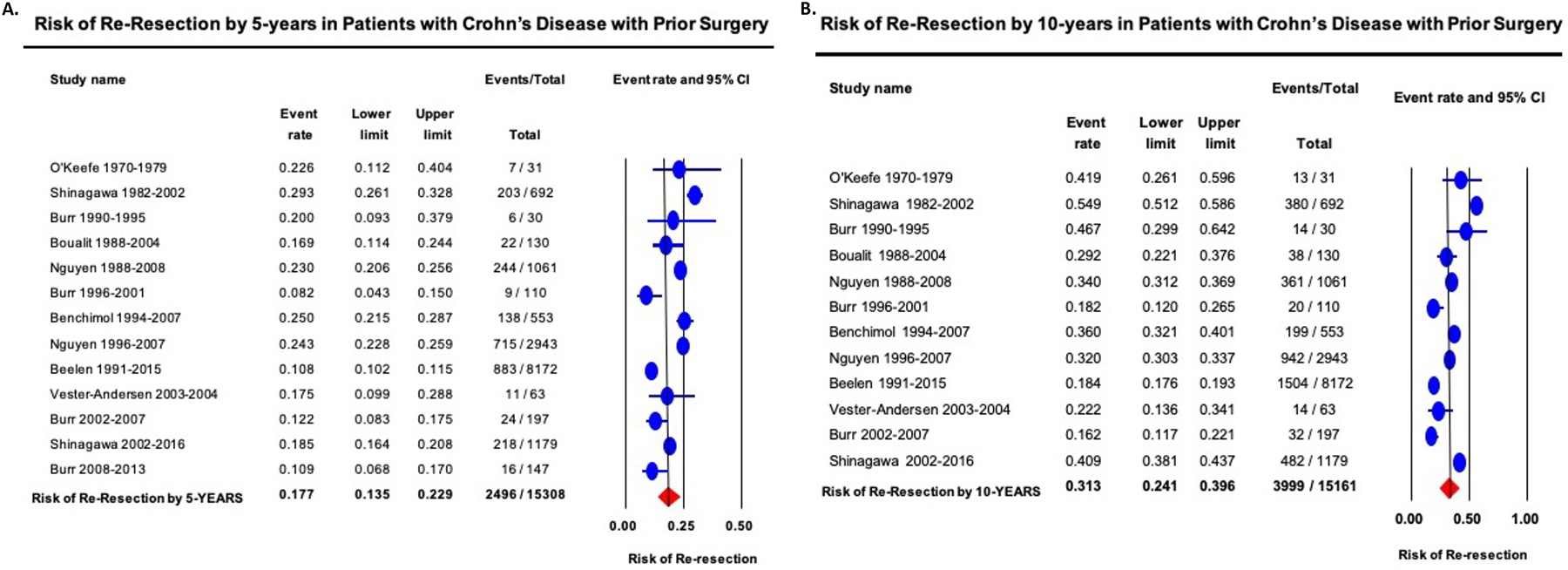
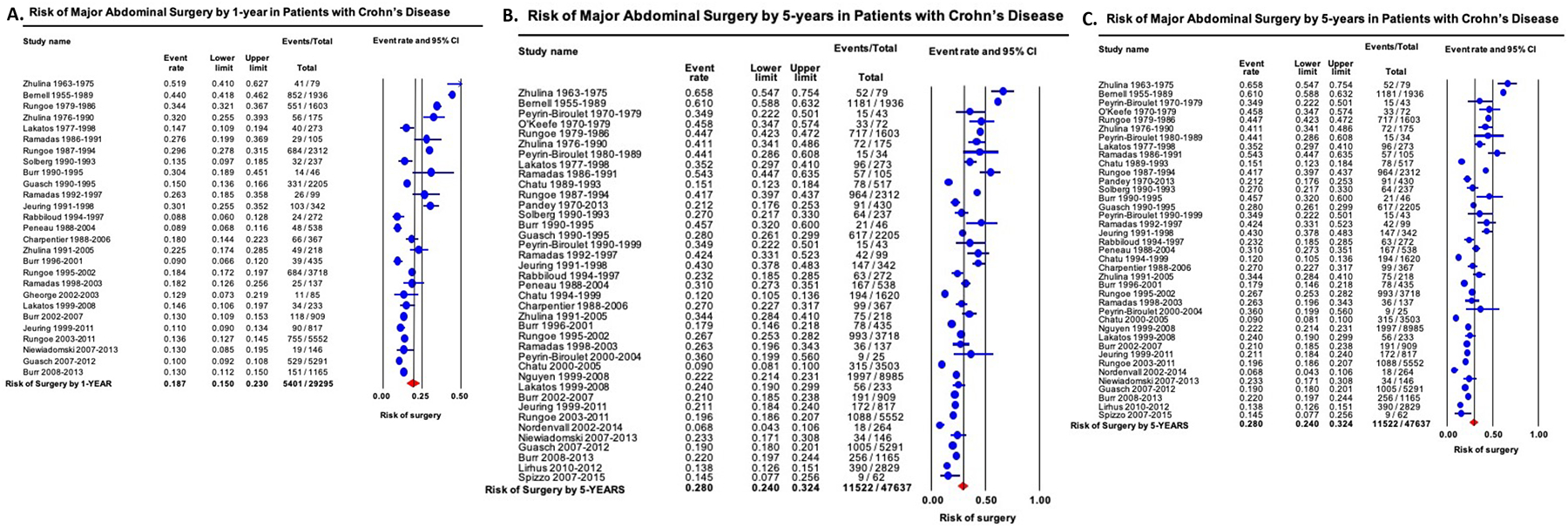
In patients with UC (26 studies), the overall 1-, 5-, and 10-year risks of colectomy was 4.0% (95% CI, 3.3-5.0), 8.8% (95% CI, 7.7-10.0), and 13.3% (95% CI, 11.3-15.5), respectively, with a decrease in risk over time (P < .001). Corresponding contemporary risks were 2.8% (95% CI, 2.0-3.9), 7.0% (95% CI, 5.7-8.6), and 9.6% (95% CI, 6.3-14.2), respectively. In patients with CD (22 studies), the overall 1-, 5-, and 10-year risk of surgery was 18.7% (95% CI, 15.0-23.0), 28.0% (95% CI, 24.0-32.4), and 39.5% (95% CI, 33.3-46.2), respectively, with a decrease in risk over time (P < .001). Corresponding contemporary risks were 12.3% (95% CI, 10.8-14.0), 18.0% (95% CI, 15.4-21.0), and 26.2% (95% CI, 23.4-29.4), respectively. In a meta-analysis of 8 studies in patients with CD with prior resection, the cumulative risk of a second resection at 5 and 10 years after the first resection was 17.7% (95% CI, 13.5-22.9) and 31.3% (95% CI, 24.1-39.6), respectively.
Patient-level risks of surgery have decreased significantly over time, with a 5-year cumulative risk of surgery of 7.0% in UC and 18.0% in CD in contemporary cohorts. This decrease may be related to early detection and/or better treatment.
我们进行了一项系统回顾和荟萃分析,以评估溃疡性结肠炎(UC)患者行结肠切除术和克罗恩病(CD)患者行原发性和再次切除术的发生率和趋势,并重点关注当代风险。
通过系统回顾,我们确定了截至 2019 年 9 月 3 日报告 UC 和 CD 患者手术累积风险的基于人群的队列研究。我们评估了 UC 患者的总体和当代(2000 年后)手术风险,并通过混合效应荟萃回归分析时间趋势。
在 UC 患者(26 项研究)中,结肠切除术的 1 年、5 年和 10 年总体风险分别为 4.0%(95%CI,3.3-5.0)、8.8%(95%CI,7.7-10.0)和 13.3%(95%CI,11.3-15.5),随着时间的推移风险呈下降趋势(P<0.001)。相应的当代风险分别为 2.8%(95%CI,2.0-3.9)、7.0%(95%CI,5.7-8.6)和 9.6%(95%CI,6.3-14.2)。在 CD 患者(22 项研究)中,手术的 1 年、5 年和 10 年总体风险分别为 18.7%(95%CI,15.0-23.0)、28.0%(95%CI,24.0-32.4)和 39.5%(95%CI,33.3-46.2),随着时间的推移风险呈下降趋势(P<0.001)。相应的当代风险分别为 12.3%(95%CI,10.8-14.0)、18.0%(95%CI,15.4-21.0)和 26.2%(95%CI,23.4-29.4)。在一项对 8 项 CD 患者既往切除术后再次切除的研究进行的荟萃分析中,首次切除术后 5 年和 10 年的第二次切除累积风险分别为 17.7%(95%CI,13.5-22.9)和 31.3%(95%CI,24.1-39.6)。
随着时间的推移,患者手术风险显著降低,UC 患者的 5 年累积手术风险为 7.0%,CD 患者为 18.0%。这种下降可能与早期发现和/或更好的治疗有关。