Division of Neurosurgery, Shizuoka Cancer Center, Nagaizumi-cho, Shizuoka, Japan.
Division of Diagnostic Pathology, Shizuoka Cancer Center, Nagaizumi-cho, Shizuoka, Japan, Japan.
Nagoya J Med Sci. 2020 Aug;82(3):533-543. doi: 10.18999/nagjms.82.3.533.
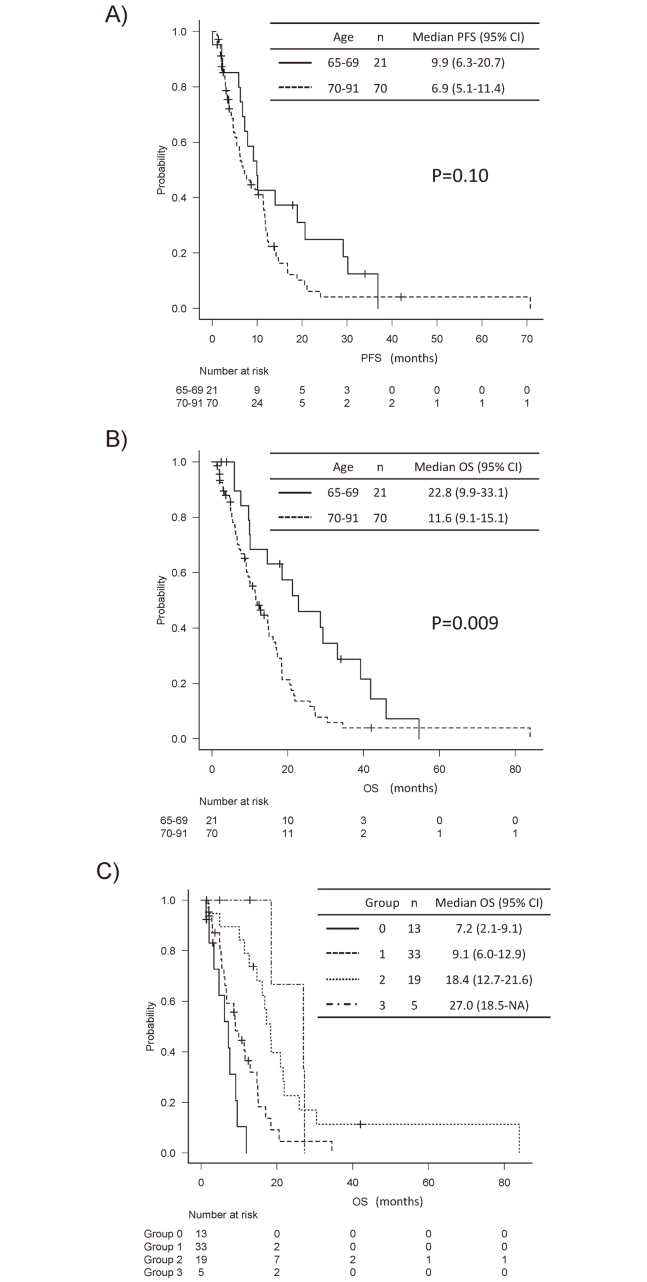
This study aimed to identify the elderly generation with the worst prognoses for high-grade astrocytoma and find independent predictors of good outcomes. We conducted a retrospective analysis of 91 patients, ≥65 years old, with anaplastic astrocytoma or glioblastoma. Progression-free survival (PFS) and overall survival (OS) were calculated using the Kaplan-Meier method and compared using log-rank test or multivariate Cox regression analysis. We included 21 (23%) and 70 (77%) patients aged 65-69 years and ≥70 years. In the two generations, significant differences were found in the Charlson comorbidity index, extent of resection, chemoradiotherapy (CRT) as adjuvant therapy, and radiation dose (all P < 0.05). The median PFS was 9.9 and 6.9 months in patients aged 65-69 and ≥70 years (P = 0.10). The median OS was 22.8 and 11.6 months in patients aged 65-69 and ≥70 years (P = 0.009). In the multivariate analyzes in patients ≥70 years, only postoperative Karnofsky performance status (KPS) scores ≥70 were significantly related to prolonged PFS (hazard ratio [HR]: 0.48, P = 0.04), and postoperative KPS, CRT as adjuvant therapy, and salvage therapy were significantly related to prolonged OS (HR: 0.45, P = 0.03, HR: 0.38, P = 0.002, and HR: 0.43, P = 0.01, respectively). In conclusion, in patients ≥70 with high-grade astrocytoma, OS was significantly shorter compared to those aged 65-69. Postoperative KPS score was significantly related to prolonged PFS and OS. Postoperative CRT and salvage therapy at recurrence may be effective in the selected elderly.
本研究旨在确定高级别星形细胞瘤预后最差的老年人群,并寻找良好预后的独立预测因素。我们对 91 名年龄≥65 岁的间变性星形细胞瘤或胶质母细胞瘤患者进行了回顾性分析。使用 Kaplan-Meier 方法计算无进展生存期(PFS)和总生存期(OS),并使用对数秩检验或多变量 Cox 回归分析进行比较。我们纳入了年龄在 65-69 岁和≥70 岁的 21 例(23%)和 70 例(77%)患者。在两代人中,Charlson 合并症指数、切除程度、放化疗(CRT)作为辅助治疗以及放疗剂量均存在显著差异(均 P<0.05)。年龄在 65-69 岁和≥70 岁的患者中位 PFS 分别为 9.9 和 6.9 个月(P=0.10)。年龄在 65-69 岁和≥70 岁的患者中位 OS 分别为 22.8 和 11.6 个月(P=0.009)。在≥70 岁患者的多变量分析中,仅术后 Karnofsky 表现状态(KPS)评分≥70 与 PFS 延长显著相关(风险比 [HR]:0.48,P=0.04),术后 KPS、CRT 作为辅助治疗和挽救性治疗与 OS 延长显著相关(HR:0.45,P=0.03;HR:0.38,P=0.002;HR:0.43,P=0.01)。总之,与 65-69 岁患者相比,≥70 岁的高级别星形细胞瘤患者 OS 显著缩短。术后 KPS 评分与 PFS 和 OS 延长显著相关。术后 CRT 和复发时的挽救性治疗可能对选择的老年患者有效。