Bezinover Dmitri, Nahouraii Lauren, Sviatchenko Alexandr, Wang Ming, Kimatian Steven, Saner Fuat H, Stine Jonathan G
Department of Anesthesiology and Perioperative Medicine, Penn State Health Milton S. Hershey Medical Center, The Pennsylvania State University, Hershey, PA.
Department of Public Health Sciences, Penn State College of Medicine, The Pennsylvania State University, Hershey, PA.
Transplant Direct. 2020 Sep 17;6(10):e604. doi: 10.1097/TXD.0000000000001050. eCollection 2020 Oct.
Our aim was to determine whether hyponatremia is associated with waiting list or posttransplantation mortality in children having liver transplantation (LT).
A retrospective analysis of the united network for organ sharing/organ procurement transplantation network database on pediatric LT performed between 1988 and 2016 was conducted. Hyponatremia was defined as a serum sodium of 130 mEq/L or below. Subjects were divided into 2 age groups: I (0-6 y old) and II (7-18 y old). Patient survival before and after LT, as well as graft survival, were compared in patients with and without hyponatremia. Multivariable Cox proportional hazards models were constructed for perioperative mortality.
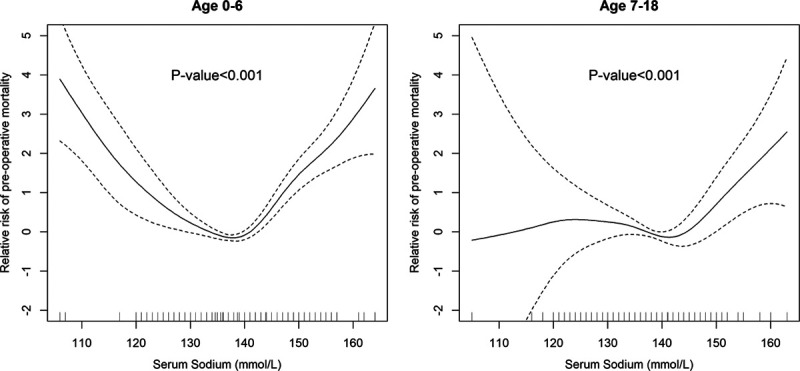
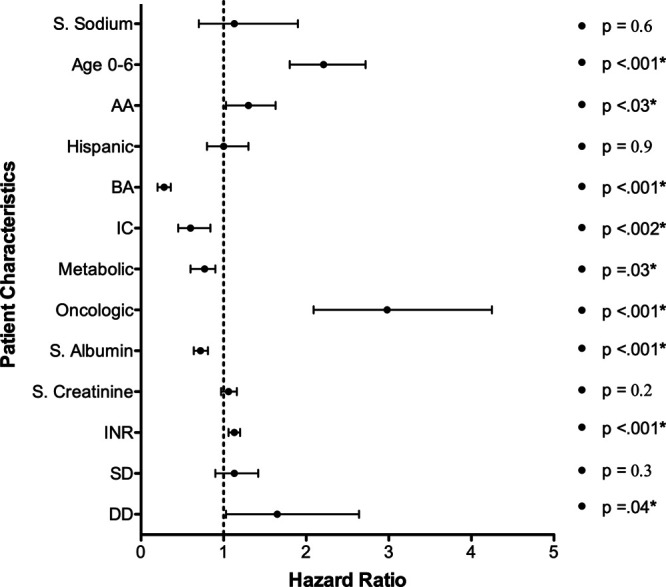
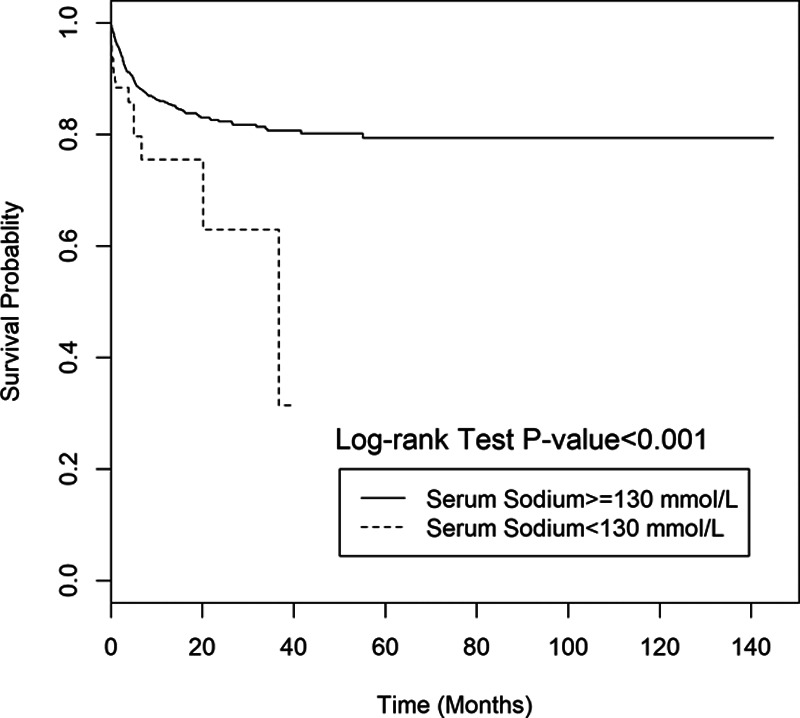
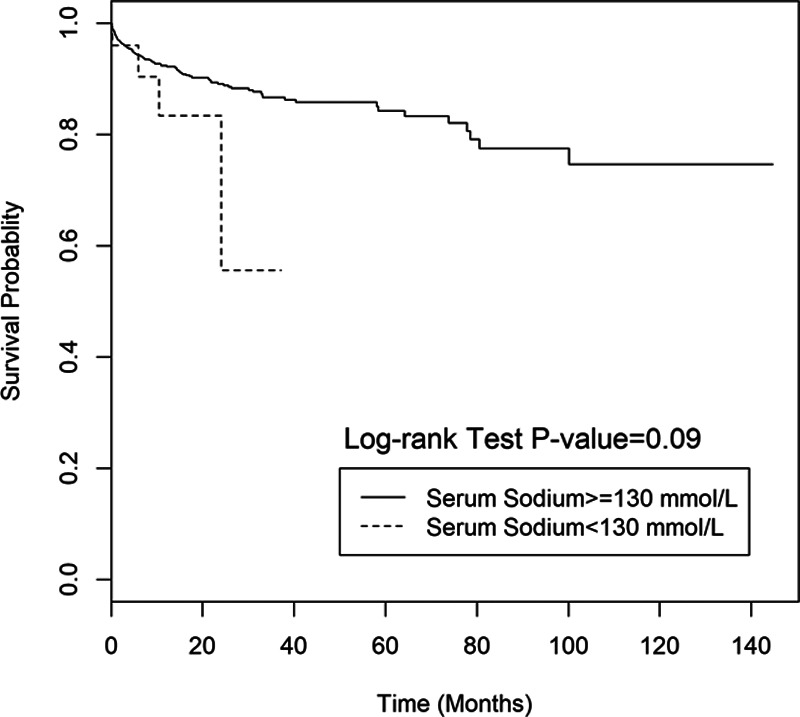
Data from 6606 children were available for analysis of waiting list mortality, and 4478 for postoperative mortality. The prevalence of hyponatremia at the time of registration was 2.8% and 3.7% at the time of LT. Waiting list mortality in patients with hyponatremia was significantly higher in group I ( < 0.001) but not in group II ( = 0.09). In group I, the relative risk of mortality adjusted to pediatric end-stage liver disease score was significantly associated with hyponatremia ( < 0.001). A sodium level below 130 mEq/L (hazard ration [HR] = 1.7), younger age (group I) (HR = 2.01), and need for dialysis (HR = 2.3) were independent predictors for increased waiting list mortality. There was no difference in overall postoperative patient or graft survival related to hyponatremia.
Hyponatremia is associated with increased waiting list mortality for pediatric LT candidates, particularly in younger children. Future studies examining incorporation of age-specific serum sodium levels into organ allocation policies in children seems warranted based on our findings.
我们的目的是确定低钠血症是否与儿童肝移植(LT)等待名单上的死亡率或移植后死亡率相关。
对1988年至2016年间进行的儿童LT的器官共享联合网络/器官获取移植网络数据库进行回顾性分析。低钠血症定义为血清钠130 mEq/L或更低。受试者分为2个年龄组:I组(0 - 6岁)和II组(7 - 18岁)。比较有和没有低钠血症的患者LT前后的患者生存率以及移植物生存率。构建多变量Cox比例风险模型用于围手术期死亡率分析。
6606名儿童的数据可用于分析等待名单死亡率,4478名可用于术后死亡率分析。登记时低钠血症的患病率为2.8%,LT时为3.7%。I组中低钠血症患者的等待名单死亡率显著更高(<0.001),但II组中无显著差异(=0.09)。在I组中,根据儿童终末期肝病评分调整后的死亡相对风险与低钠血症显著相关(<0.001)。钠水平低于130 mEq/L(风险比[HR]=1.7)、年龄较小(I组)(HR=2.01)和需要透析(HR=2.3)是等待名单死亡率增加的独立预测因素。与低钠血症相关的总体术后患者或移植物生存率没有差异。
低钠血症与儿童LT候选者等待名单死亡率增加相关,尤其是年幼儿童。基于我们的研究结果,未来研究将特定年龄的血清钠水平纳入儿童器官分配政策似乎是有必要的。