Department of General Surgery, Vanderbilt University Medical Center, Nashville, TN, USA.
School of Medicine, Meharry Medical College, Nashville, TN, USA.
Surg Endosc. 2021 Nov;35(11):6081-6088. doi: 10.1007/s00464-020-08101-6. Epub 2020 Nov 2.
Surgical society guidelines have recommended changing the treatment strategy for early esophageal cancer during the novel coronavirus (COVID-19) pandemic. Delaying resection can allow for interim disease progression, but the impact of this delay on mortality is unknown. The COVID-19 infection rate at which immediate operative risk exceeds benefit is unknown. We sought to model immediate versus delayed surgical resection in a T1b esophageal adenocarcinoma.
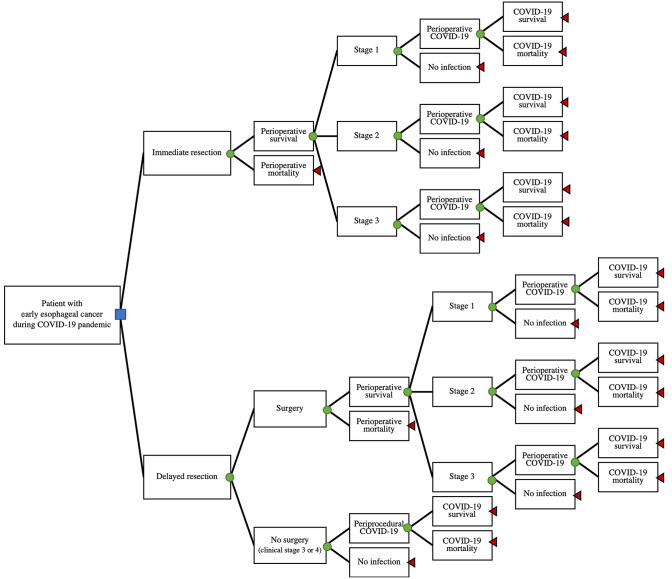
A decision analysis model was developed, and sensitivity analyses performed. The base case was a 65-year-old male smoker presenting with cT1b esophageal adenocarcinoma scheduled for esophagectomy during the COVID-19 pandemic. We compared immediate surgical resection to delayed resection after 3 months. The likelihood of key outcomes was derived from the literature where available. The outcome was 5-year overall survival.
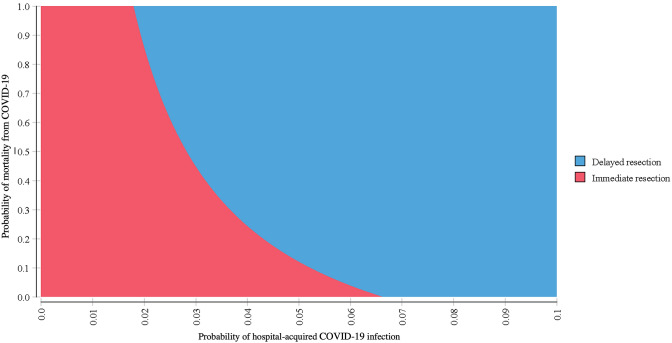
Proceeding with immediate esophagectomy for the base case scenario resulted in slightly improved 5-year overall survival when compared to delaying surgery by 3 months (5-year overall survival 0.74 for immediate and 0.73 for delayed resection). In sensitivity analyses, a delayed approach became preferred when the probability of perioperative COVID-19 infection increased above 7%.
Immediate resection of early esophageal cancer during the COVID-19 pandemic did not decrease 5-year survival when compared to resection after 3 months for the base case scenario. However, as the risk of perioperative COVID-19 infection increases above 7%, a delayed approach has improved 5-year survival. This balance should be frequently re-examined by surgeons as infection risk changes in each hospital and community throughout the COVID-19 pandemic.
外科协会指南建议在新型冠状病毒(COVID-19)大流行期间改变早期食管癌的治疗策略。延迟切除可以允许疾病的中间进展,但这种延迟对死亡率的影响尚不清楚。目前尚不清楚立即进行手术的风险超过获益的 COVID-19 感染率。我们试图在 T1b 食管腺癌患者中对立即手术与延迟手术进行建模。
我们开发了一个决策分析模型,并进行了敏感性分析。基础病例为一名 65 岁男性吸烟者,患有 cT1b 食管腺癌,在 COVID-19 大流行期间计划接受食管切除术。我们比较了立即手术切除与 3 个月后延迟切除。关键结果的可能性可从现有文献中获得。结果是 5 年总生存率。
与延迟 3 个月手术相比,对于基础病例,立即进行食管切除术可略微提高 5 年总生存率(立即手术的 5 年总生存率为 0.74,延迟手术为 0.73)。在敏感性分析中,当围手术期 COVID-19 感染的概率增加到 7%以上时,延迟方法成为首选。
在 COVID-19 大流行期间,与延迟 3 个月手术相比,立即切除早期食管癌并没有降低 5 年生存率。然而,随着围手术期 COVID-19 感染的风险增加到 7%以上,延迟方法提高了 5 年生存率。随着 COVID-19 大流行期间每个医院和社区的感染风险发生变化,外科医生应定期重新评估这种平衡。