Torres Maria E, Brolin Mary, Panas Lee, Ritter Grant, Hodgkin Dominic, Lee Margaret, Merrick Elizabeth, Horgan Constance, Hopwood Jonna C, Gewirtz Andrea, De Marco Natasha, Lane Nancy
Brandeis University, Heller School for Social Policy and Management, Waltham, MA, 02453, USA.
Smith College School for Social Work, Lilly Hall, Northampton, MA, 01060, USA.
BMC Health Serv Res. 2020 Nov 3;20(1):1004. doi: 10.1186/s12913-020-05861-8.
Acute 24-h detoxification services (detox) are necessary but insufficient for many individuals working towards long-term recovery from opiate, alcohol or other drug addiction. Longer engagement in substance use disorder (SUD) treatment can lead to better health outcomes and reductions in overall healthcare costs. Connecting individuals with post-detox SUD treatment and supportive services is a vital next step. Toward this end, the Massachusetts Medicaid program reimburses Community Support Program staff (CSPs) to facilitate these connections. CSP support services are typically paid on a units-of-service basis. As part of a larger study testing health care innovations, one large Medicaid insurer developed a new cadre of workers, called Recovery Support Navigators (RSNs). RSNs performed similar tasks to CSPs but received more extensive training and coaching and were paid an experimental case rate (a flat negotiated reimbursement). This sub-study evaluates the feasibility and impact of case rate payments for RSN services as compared to CSP services paid fee-for-service.
We analyzed claims data and RSN service data for a segment of the Massachusetts Medicaid population who had more than one detox admission in the last year and also engaged in post-discharge CSP or RSN services. Qualitative data from key informant interviews and Learning Collaboratives with CSPs and RSNs supplemented the findings.
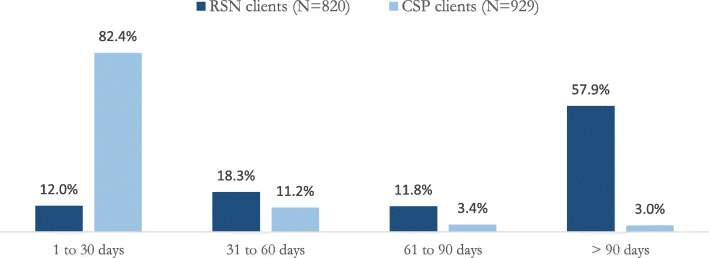
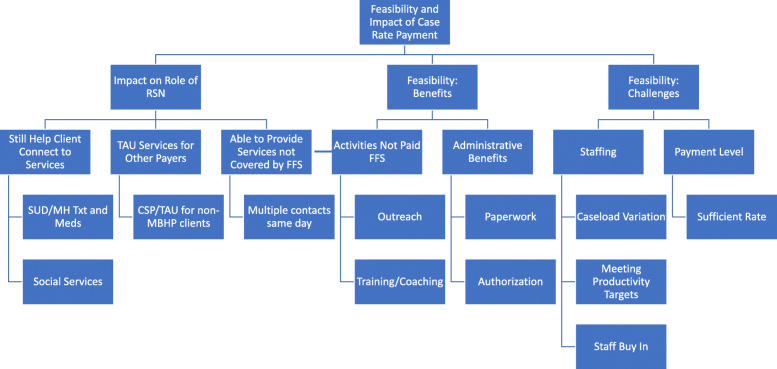
Clients receiving RSN services under the case rate utilized the service significantly longer than clients receiving CSP services under unit-based billing. This resulted in a lower average cost per member per month for RSN clients. However, when calculating total SUD treatment costs per member, RSN client costs were 50% higher than CSP client costs. Provider organizations employing RSNs successfully implemented case rate billing. Benefits included allowing time for outreach efforts and training and coaching, activities not paid under the unit-based system. Yet, RSNs identified staffing and larger systems level challenges to consider when using a case rate payment model.
Addiction is a chronic disease that requires long-term investments. Case rate billing offers a promising option for payers and providers as it promotes continued engagement with service providers. To fully realize the benefits of case rate billing, however, larger systems level changes are needed.
对于许多致力于从阿片类药物、酒精或其他药物成瘾中实现长期康复的人来说,急性24小时戒毒服务是必要的,但并不充分。更长时间地参与物质使用障碍(SUD)治疗可带来更好的健康结果,并降低总体医疗成本。将个人与戒毒后的SUD治疗及支持性服务联系起来是至关重要的下一步。为此,马萨诸塞州医疗补助计划向社区支持项目工作人员(CSP)报销费用,以促进这些联系。CSP支持服务通常按服务单元计费。作为一项测试医疗创新的大型研究的一部分,一家大型医疗补助保险公司组建了一支新的工作人员队伍,称为康复支持导航员(RSN)。RSN执行与CSP类似的任务,但接受了更广泛的培训和指导,并按实验性病例费率(协商确定的固定报销费用)支付薪酬。本子研究评估了与按服务收费的CSP服务相比,按病例费率支付RSN服务费用的可行性和影响。
我们分析了马萨诸塞州医疗补助人群中一部分人的理赔数据和RSN服务数据,这些人在过去一年中有不止一次戒毒入院记录,并且在出院后接受了CSP或RSN服务。来自关键信息提供者访谈以及与CSP和RSN的学习合作组织的定性数据补充了研究结果。
按病例费率接受RSN服务的客户使用该服务的时间明显长于按单元计费接受CSP服务的客户。这导致RSN客户的每月人均成本较低。然而,在计算每位成员的SUD治疗总成本时,RSN客户的成本比CSP客户的成本高50%。雇佣RSN的服务提供机构成功实施了病例费率计费。好处包括有时间进行外展工作以及培训和指导,这些活动在基于单元的系统下是不付费的。然而,RSN指出了在使用病例费率支付模式时需要考虑的人员配备和更大系统层面的挑战。
成瘾是一种需要长期投入的慢性疾病。病例费率计费为支付方和服务提供机构提供了一个有前景的选择,因为它促进了与服务提供者的持续接触。然而,要充分实现病例费率计费的好处,需要在更大的系统层面进行变革。