Oster Yonatan, Cohen Matan J, Dresner-Pollak Rivka, Szalat Auryan, Elinav Hila
Hadassah AIDS Center, Department of Clinical Microbiology and Infectious Diseases, Hadassah Hebrew University Medical Center, Jerusalem, Israel.
Clalit Health Services, Jerusalem District, affiliated with the School of Medicine, Hebrew University, Jerusalem, Israel.
Bone Rep. 2020 Oct 16;13:100727. doi: 10.1016/j.bonr.2020.100727. eCollection 2020 Dec.
Accelerated bone loss and osteoporosis are multifactorial comorbidities related to HIV and its treatments; however, their mechanisms remain elusive. Identifying HIV treatments that are differentially linked to osteoporosis risk, and clinical factors associated with HIV-related osteoporosis may enable optimizing anti-retroviral treatment (ART) and anti-osteoporosis therapy in preventing or treating this debilitating complication. This study aims to evaluate the dynamics of bone turnover markers after initiation of two commonly used antiretroviral regimens.
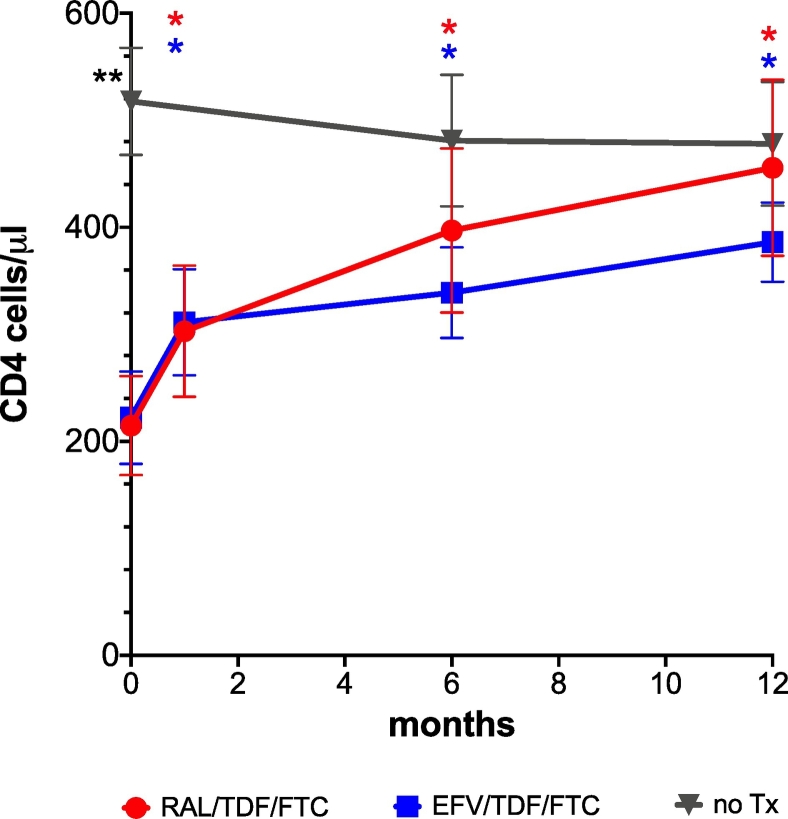
A prospective matched cohort study. Thirty treatment-naïve male patients (mean age 40 ± 10y) who initiated treatment with truvada (tenofovir disoproxil fumarate (TDF)/emtricitabine (FTC)) + raltegravir or TDF/FTC + efavirenz were included in the study. Control group included 15 treatment-naive HIV patients. Serum morning fasting level of P1NP and CTX were measured 0, 1, 6, and 12 months after treatment initiation in the two study groups, and at 0, 6 and 12 months in the control group.
In both treatment groups, but not in the control group, both markers increased significantly over time with no difference in BTM between patients treated with raltegravir or efavirenz. Levels of P1NP were statistically higher at 6 and 12 months after treatment initiation in both treatment groups compared to the controls, while CTX during treatment increased in both treatment groups but was significantly higher only in the raltegravir treatment group after 12 months. The ratio of area under the curve of P1NP/CTX correlated with CD4 increment.
Treatment initiation with raltegravir or efavirenz combined with TDF/FTC is associated with increased bone turnover. Thus, therapy that optimize bone turnover is needed to reduce bone loss at this vulnerable period and improve long-term bone health.
骨质流失加速和骨质疏松是与人类免疫缺陷病毒(HIV)及其治疗相关的多因素合并症;然而,其机制仍不清楚。确定与骨质疏松风险有不同关联的HIV治疗方法以及与HIV相关骨质疏松症相关的临床因素,可能有助于优化抗逆转录病毒治疗(ART)和抗骨质疏松治疗,以预防或治疗这种使人衰弱的并发症。本研究旨在评估两种常用抗逆转录病毒治疗方案开始后骨转换标志物的动态变化。
一项前瞻性匹配队列研究。30例初治男性患者(平均年龄40±10岁)开始使用特鲁瓦达(替诺福韦酯(TDF)/恩曲他滨(FTC))+拉替拉韦或TDF/FTC+依非韦伦进行治疗,被纳入研究。对照组包括15例初治HIV患者。在两个研究组治疗开始后的0、1、6和12个月,以及对照组的0、6和12个月,测量血清空腹P1NP和CTX水平。
在两个治疗组中,但不在对照组中,两种标志物均随时间显著增加,接受拉替拉韦或依非韦伦治疗的患者之间的骨转换标志物无差异。与对照组相比,两个治疗组在治疗开始后6个月和12个月时P1NP水平在统计学上更高,而治疗期间两个治疗组的CTX均升高,但仅在拉替拉韦治疗组12个月后显著更高。P1NP/CTX曲线下面积之比与CD4增加相关。
拉替拉韦或依非韦伦联合TDF/FTC开始治疗与骨转换增加有关。因此,需要优化骨转换的治疗方法,以减少这一脆弱时期的骨质流失,改善长期骨骼健康。