Taguchi Yuka, Hara Takanobu, Tamura Hiroaki, Ogiku Masahito, Watahiki Mana, Takagi Toru, Harada Takashi, Miyazaki Shinichiro, Hayashi Tadataka, Kanai Toshikazu, Mori Hiroki, Ozawa Takachika, Nishiwaki Yoshiro
Department of Gastroenterological Surgery, Hamamatsu Medical Center, 328 Tomitsukacho, Naka-ku, Hamamatsu city, Shizuoka, 432-8580, Japan.
Department of Surgery, Nagasaki University Graduate School of Biomedical Sciences, 1-7-1 Sakamoto, Nagasaki City, Nagasaki, 852-8501, Japan.
Surg Case Rep. 2020 Nov 13;6(1):287. doi: 10.1186/s40792-020-01067-6.
Solitary fibrous tumors (SFTs) are rare tumors, mostly derived from connective tissue mesenchymal cells that arise from the pleura. There are very few reports of primary pancreatic SFT. Preoperative diagnosis is difficult owing to the lack of distinctive radiological findings. We report a case of pancreatic SFT with particularly rare malignant findings.
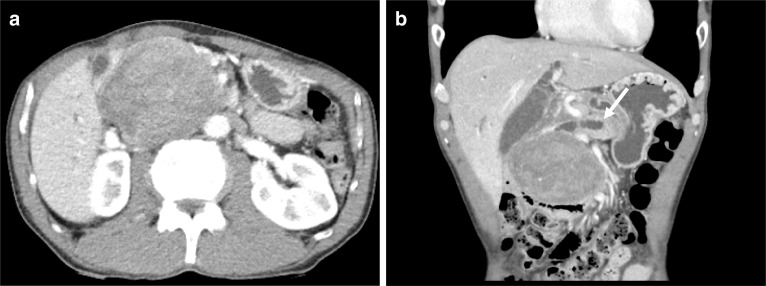
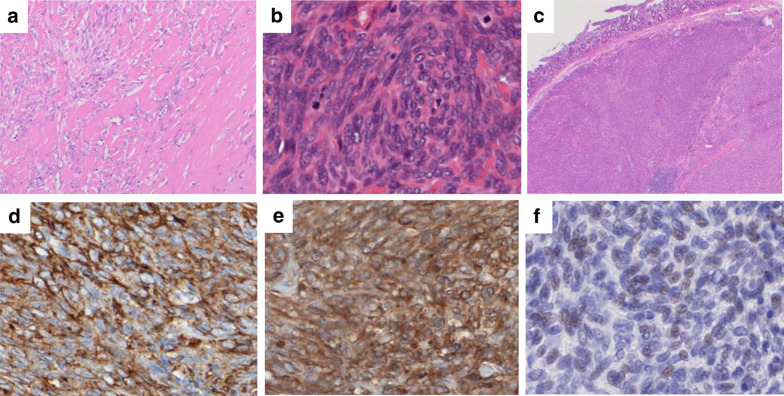
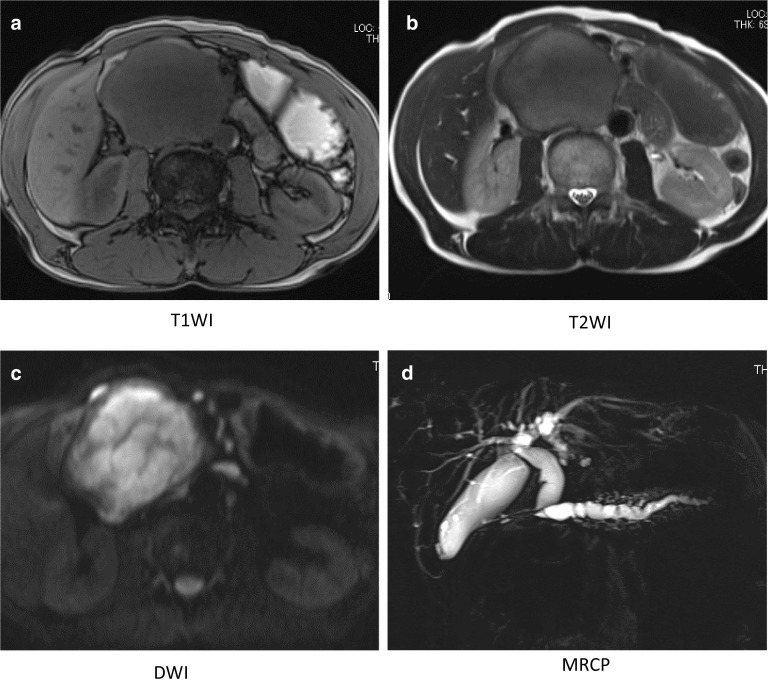
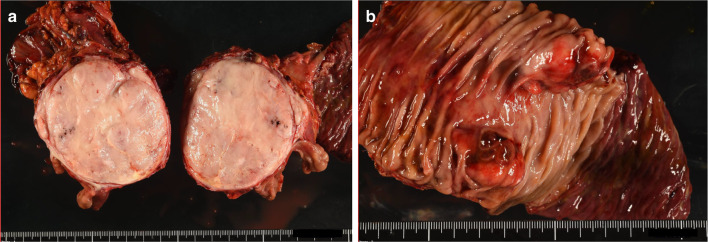
A 60-year-old man was referred to the hospital because of a right upper quadrant mass and abnormal liver function test results. Contrast-enhanced computed tomography (CT) showed a well-defined enhanced tumor measuring approximately 8 cm in the pancreatic head. Magnetic resonance imaging (MRI) showed T1WI hypointensity, T2WI hyperintensity, and DWI hyperintensity. The main pancreatic duct and common bile duct were dilated owing to obstruction by the tumor. The following tumor markers were mildly elevated: carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), SPan-1, and DUPAN-2. The histological diagnosis obtained by endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) was negative for pancreatic ductal carcinoma, malignant lymphoma and neuroendocrine tumor, suggesting the possibility of mesenchymal tumor, but the diagnosis was not confirmed. The patient was judged suitable for surgery and underwent subtotal stomach-preserving pancreatoduodenectomy with D2 lymph node dissection. On histopathological examination of the resected specimen, infiltrating spindle-shaped cells had proliferated, containing numerous mitotic figures, with necrotic findings inside the tumor. Immunostaining was positive for cluster of differentiation-34 (CD34), B cell CLL/lymphoma-2 (Bcl-2), and signal transducer and activator of transcription (STAT6). On the basis of these findings, a diagnosis of malignant pancreatic SFT was made. The patient remains free of recurrent disease after 12 months of follow-up without adjuvant therapy and he is being carefully followed up as an outpatient.
We experienced a case of malignant pancreatic head SFT. Immunohistochemical staining of the extracted specimens was useful for diagnosis.
孤立性纤维性肿瘤(SFTs)是罕见肿瘤,大多起源于胸膜的结缔组织间充质细胞。原发性胰腺SFT的报道极少。由于缺乏独特的影像学表现,术前诊断困难。我们报告一例具有特别罕见恶性表现的胰腺SFT病例。
一名60岁男性因右上腹肿块及肝功能检查结果异常被转诊至我院。增强计算机断层扫描(CT)显示胰头有一个边界清晰的强化肿瘤,大小约8厘米。磁共振成像(MRI)显示T1加权成像(T1WI)低信号、T2加权成像(T2WI)高信号及扩散加权成像(DWI)高信号。主胰管和胆总管因肿瘤阻塞而扩张。以下肿瘤标志物轻度升高:癌胚抗原(CEA)、糖类抗原19-9(CA19-9)、SPan-1和DUPAN-2。经内镜超声引导下细针穿刺活检(EUS-FNA)获得的组织学诊断排除了胰腺导管癌、恶性淋巴瘤和神经内分泌肿瘤,提示间叶性肿瘤的可能性,但诊断未得到证实。该患者被判定适合手术,接受了保留胃的胰十二指肠次全切除术及D2淋巴结清扫术。对切除标本进行组织病理学检查时,可见浸润性梭形细胞增生,有大量有丝分裂象,肿瘤内部有坏死表现。免疫组化染色显示分化簇34(CD34)、B细胞淋巴瘤/白血病-2(Bcl-2)及信号转导和转录激活因子(STAT6)呈阳性。基于这些发现,诊断为恶性胰腺SFT。患者在未接受辅助治疗的情况下随访12个月无疾病复发,目前作为门诊患者正在接受密切随访。
我们遇到一例恶性胰头SFT病例。提取标本的免疫组化染色对诊断有帮助。