Tözün Ismail Remzi, Ozden Vahit Emre, Dikmen Goksel, Karaytuğ Kayahan
Department of Orthopaedic Surgery and Traumatology, Acibadem Mehmet Ali Aydınlar University, School of Medicine, Acibadem Maslak Hospital, Sarıyer/Istanbul, Turkey.
EFORT Open Rev. 2020 Oct 26;5(10):672-683. doi: 10.1302/2058-5241.5.190069. eCollection 2020 Oct.
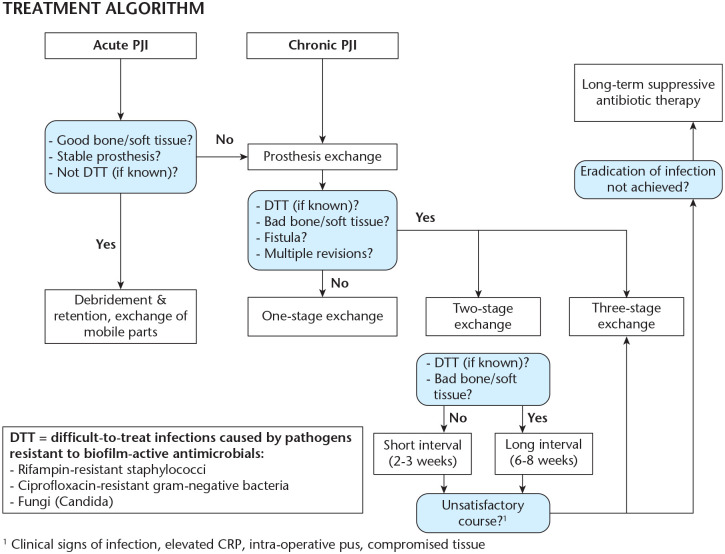
Essential treatment methods for infected knee arthroplasty involve DAIR (debridement, antibiotics, and implant retention), and one and two-stage exchange arthroplasty.Aggressive debridement with the removal of all avascular tissues and foreign materials that contain biofilm is mandatory for all surgical treatment modalities.DAIR is a viable option with an acceptable success rate and can be used as a first surgical procedure for patients who have a well-fixed, functioning prosthesis without a sinus tract for acute-early or late-hematogenous acute infections with no more than four weeks (most favourable being < seven days) of symptoms. Surgeons must focus on the isolation of the causative organism with sensitivities to bactericidal treatment as using one-stage exchange.One-stage exchange is indicated when the patients have:minimal bone loss/soft tissue defect allowing primary wound closure,easy to treat micro-organisms,absence of systemic sepsis andabsence of extensive comorbidities.There are no validated serum or synovial biomarkers to determine optimal timing of re-implantation for two-stage exchange.Antibiotic-free waiting intervals and joint aspiration before the second stage are no longer recommended. The decision to perform aspiration should be made based on the index of suspicion for persistent infection.Re-implantation can be performed when the treating medical team feels that the clinical signs of infection are under control and serological tests are trending downwards. Cite this article: 2020;5:672-683. DOI: 10.1302/2058-5241.5.190069.
感染性膝关节置换术的基本治疗方法包括清创、抗生素应用及假体保留(DAIR),以及一期和二期翻修置换术。对于所有手术治疗方式而言,积极清创并清除所有含生物膜的无血管组织和异物是必不可少的。DAIR是一种可行的选择,成功率尚可,可作为初次手术方法用于假体固定良好、功能正常、无窦道、症状持续时间不超过四周(最理想的是<7天)的急性早期或晚期血源性急性感染患者。外科医生在进行一期翻修时必须注重分离致病微生物并确定其对杀菌治疗的敏感性。当患者具备以下情况时可考虑一期翻修:骨量丢失/软组织缺损最小,能够一期缝合伤口;微生物易于治疗;无全身脓毒症;无广泛合并症。目前尚无经过验证的血清或滑膜生物标志物来确定二期翻修的最佳再植入时机。不再推荐二期手术前无抗生素的等待期和关节穿刺。是否进行穿刺应根据对持续感染的怀疑指数来决定。当治疗团队认为感染的临床症状得到控制且血清学检查呈下降趋势时,可进行再植入。引用本文:2020;5:672 - 683。DOI: 10.1302/2058 - 5241.5.190069。