Mansoori Huma, Faraz Maria, Qadir Hira, Rashid Anila, Ali Maria
Pathology, Dow University of Health Sciences, Karachi, PAK.
Health Sciences, McMaster University, Ontario, CAN.
Cureus. 2020 Oct 17;12(10):e11009. doi: 10.7759/cureus.11009.
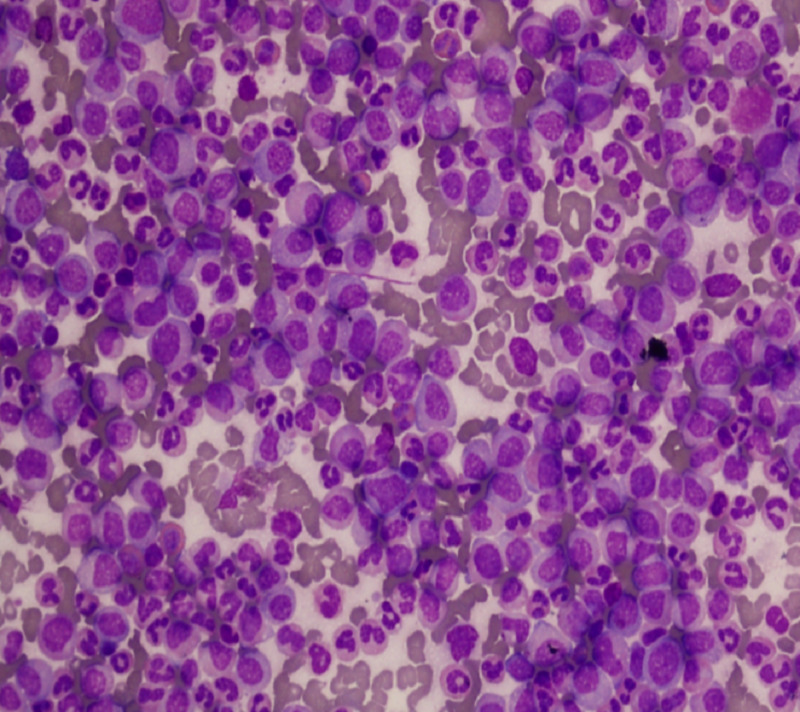
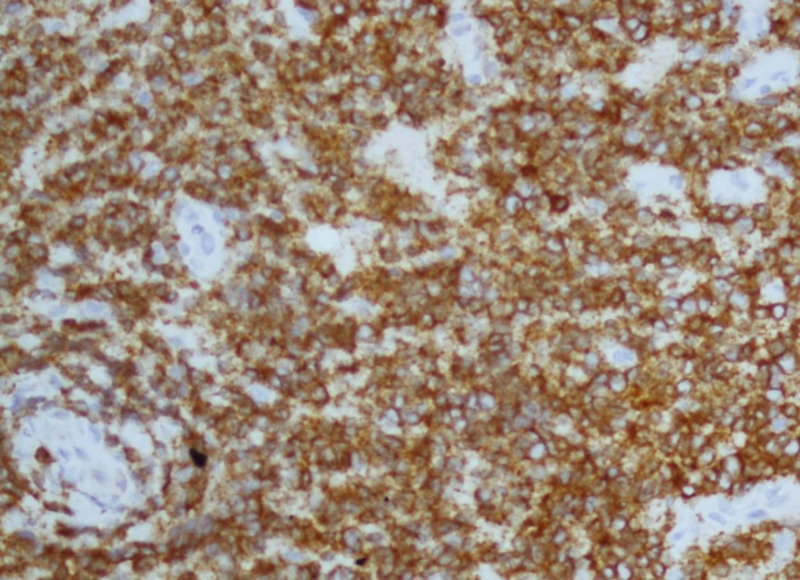
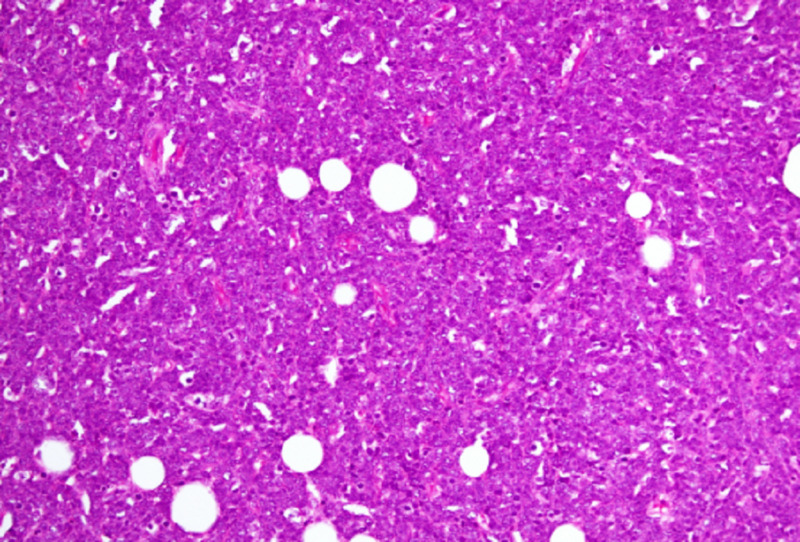
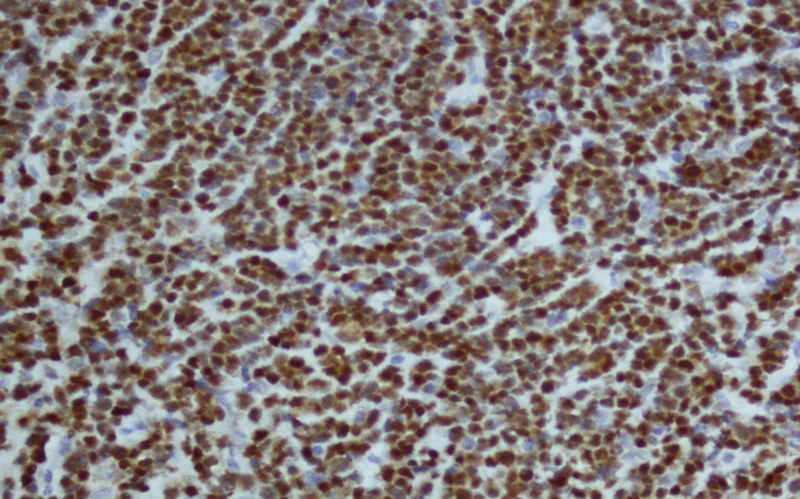
Chronic myeloid leukemia (CML) is a myeloproliferative disorder characterized by immature granulocytes in peripheral blood and bone marrow. In 95% of cases, it is always due to the presence of Philadelphia chromosome characterized by the presence of reciprocal translocation between chromosome 9 and 22. However, in 7% -17% of individuals, extramedullary proliferation also occurs, either in skin, lymph nodes, bone or central nervous system (CNS), which could be either myeloid, lymphoid or mixed progenitor in origin. The present case is of a 23-year-old male who presented with lower limb weakness, bowel and urinary incontinence. His complete blood count (CBC) findings showed a raised white blood count (WBC) of 408 X 10E9/L. Peripheral film, bone marrow biopsy and immunohistochemistry showed findings consistent with CML in chronic phase. Bone marrow cytogenetic revealed the presence of Philadelphia chromosome. Simultaneously, magnetic resonance imaging (MRI) was done which revealed extradural mass at L1-L3 level; histopathological and immunohistochemistry findings showed features compatible with precursor B cell lymphoblastic lymphoma. His cerebrospinal fluid (CSF) cytology revealed similar blast cells. This extramedullary presence of lymphoid blast cells in the CNS put the patient in the rare entity of CML in blast crisis. He was started on tablet nilotinib and also received multiple cycles of intrathecal chemotherapy with cytosar, methotrexate and hydrocortisone. He also underwent radiotherapy of extradural mass. His lower limb weakness improved dramatically. However, after receiving the fourth cycle of intrathecal therapy, the patient died consequent to neutropenic sepsis. Extramedullary blast crisis in CML has a poor prognosis. Any patient with CML, presenting with CNS symptoms or lymph node enlargement should be thoroughly investigated for extramedullary blast crisis, as there is a considerable change in management and prognosis from the prototype CML in chronic phase.
慢性髓性白血病(CML)是一种骨髓增殖性疾病,其特征为外周血和骨髓中存在未成熟粒细胞。在95%的病例中,该病总是由费城染色体导致,其特征是9号染色体和22号染色体之间存在相互易位。然而,在7% - 17%的个体中,还会发生髓外增殖,可出现在皮肤、淋巴结、骨骼或中枢神经系统(CNS),其起源可能是髓系、淋巴系或混合祖细胞系。本病例为一名23岁男性,表现为下肢无力、大小便失禁。他的全血细胞计数(CBC)结果显示白细胞计数(WBC)升高至408×10⁹/L。外周血涂片、骨髓活检和免疫组化结果显示与慢性期CML一致。骨髓细胞遗传学检查发现存在费城染色体。同时,进行了磁共振成像(MRI)检查,结果显示L1 - L3水平存在硬膜外肿块;组织病理学和免疫组化结果显示与前体B细胞淋巴母细胞淋巴瘤相符。他的脑脊液(CSF)细胞学检查发现了类似的原始细胞。CNS中这种淋巴母细胞的髓外存在使该患者处于CML急变期这一罕见情况。他开始服用尼洛替尼片剂,并接受了多个周期的鞘内化疗,使用了阿糖胞苷、甲氨蝶呤和氢化可的松。他还接受了硬膜外肿块的放射治疗。他的下肢无力症状显著改善。然而,在接受第四个周期的鞘内治疗后,患者因中性粒细胞减少性败血症死亡。CML的髓外急变期预后较差。任何患有CML且出现CNS症状或淋巴结肿大的患者都应彻底检查是否存在髓外急变期,因为与慢性期的典型CML相比,其治疗和预后有相当大的变化。