Department Clinical Pharmacology and Pharmacoepidemiology, University Hospital Heidelberg, Heidelberg, Germany.
Department of Medical Oncology, National Center for Tumor Diseases, Heidelberg, Germany.
Clin Transl Sci. 2021 Mar;14(2):487-491. doi: 10.1111/cts.12921. Epub 2020 Nov 22.
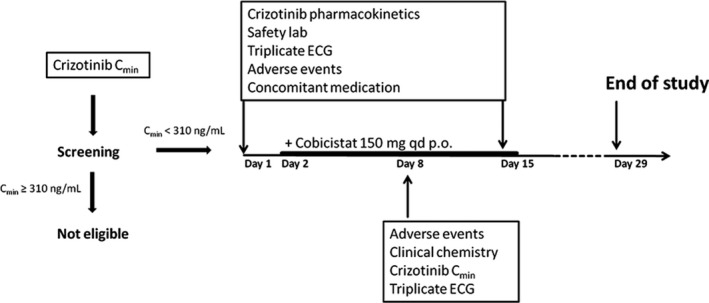
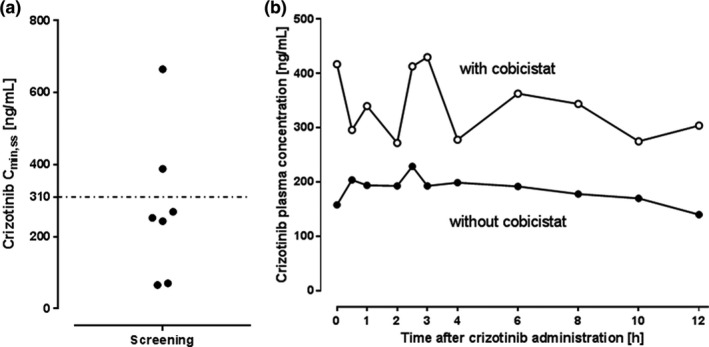
The inhibitor of anaplastic lymphoma kinase (ALK) crizotinib significantly increases survival in patients with ALK-positive non-small cell lung cancer (NSCLC). When evaluating crizotinib pharmacokinetics (PKs) in patients taking the standard flat oral dose of 250 mg b.i.d., interindividual PK variability is substantial and patient survival is lower in the quartile with the lowest steady-state trough plasma concentrations (C ), suggesting that concentrations should be monitored and doses individualized. We investigated whether the CYP3A inhibitor cobicistat increases C of the CYP3A substrate crizotinib in patients with low exposure. Patients with ALK-positive NSCLC of our outpatient clinic treated with crizotinib were enrolled in a phase I trial (EudraCT 2016-002187-14, DRKS00012360) if crizotinib C was below 310 ng/mL and treated with cobicistat for 14 days. Crizotinib plasma concentration profiles were established before and after a 14-day co-administration of cobicistat to construct the area under the plasma concentration-time curve in the dosing interval from zero to 12 hours (AUC ). Patients were also monitored for adverse events by physical examination, laboratory tests, and 12-lead echocardiogram. Enrolment was prematurely stopped because of the approval of alectinib, a next-generation ALK-inhibitor with superior efficacy. In the only patient enrolled, cobicistat increased C from 158 ng/mL (before cobicistat) to 308 ng/mL (day 8) and 417 ng/mL (day 14 on cobicistat), concurrently the AUC increased by 78% from 2,210 ng/mLh to 3,925 ng/mLh. Neither safety signals nor serious adverse events occurred. Pharmacoenhancement with cobicistat as an alternative for dose individualisation for patients with NSCLC with low crizotinib exposure appears to be safe and is cost-effective and feasible.
间变性淋巴瘤激酶 (ALK) 抑制剂克唑替尼显著提高了 ALK 阳性非小细胞肺癌 (NSCLC) 患者的生存率。在评估接受标准 250mg 每日两次平口剂量的患者的克唑替尼药代动力学 (PK) 时,个体间 PK 变异性很大,并且在稳态谷血浆浓度 (C ) 最低的四分位数中患者的生存率较低,表明应监测浓度并个体化剂量。我们研究了 CYP3A 抑制剂考比司他是否会增加低暴露患者中 CYP3A 底物克唑替尼的 C 。如果克唑替尼 C 低于 310ng/mL,并且我们门诊的 ALK 阳性 NSCLC 患者接受克唑替尼治疗,则参加一项 I 期试验(EudraCT 2016-002187-14,DRKS00012360),并接受考比司他治疗 14 天。在考比司他联合治疗 14 天后,建立克唑替尼的血浆浓度曲线下面积,从零时到 12 小时(AUC )。还通过体格检查、实验室检查和 12 导联心电图监测患者的不良事件。由于下一代 ALK 抑制剂阿来替尼的疗效优于克唑替尼,该试验提前停止入组。在唯一入组的患者中,考比司他将 C 从 158ng/mL(考比司他之前)增加到 308ng/mL(考比司他第 8 天)和 417ng/mL(考比司他第 14 天),同时 AUC 从 2210ng/mLh 增加到 3925ng/mLh,增加了 78%。既没有出现安全信号,也没有发生严重不良事件。考比司他作为一种替代药物,用于增加低克唑替尼暴露的 NSCLC 患者的剂量个体化,似乎是安全且具有成本效益和可行性的。