Lai Marcus Kin Long, Cheung Prudence Wing Hang, Samartzis Dino, Cheung Jason Pui Yin
Department of Orthopaedics and Traumatology, 25809The University of Hong Kong, Pokfulam, Hong Kong SAR, China.
Department of Orthopaedic Surgery, 2468RUSH University Medical Center, Chicago, IL, USA.
Global Spine J. 2022 Jul;12(6):1084-1090. doi: 10.1177/2192568220975384. Epub 2020 Nov 23.
Cross-sectional study.
To define multilevel lumbar developmental spinal stenosis (DSS) using a composite score model and to determine its prevalence.
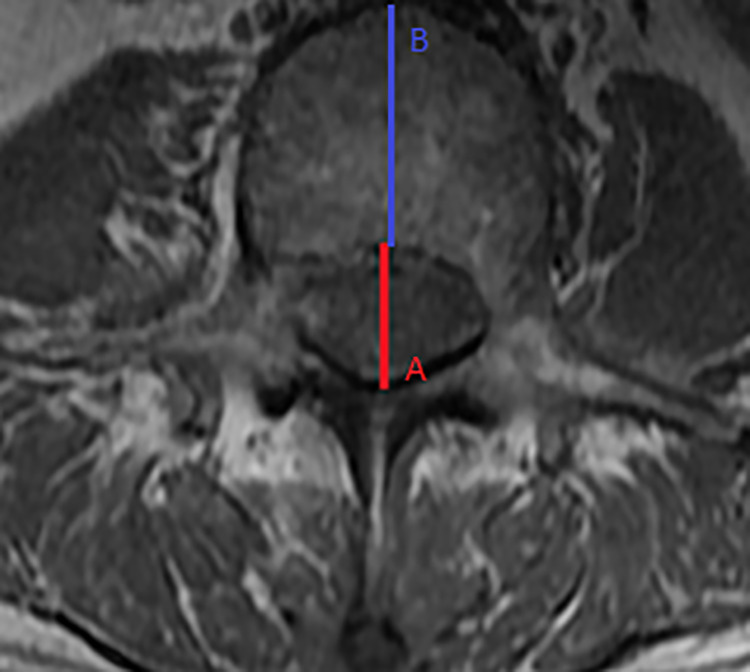
This was a cohort study of 2385 openly recruited subjects with lumbosacral (L1-S1) MRIs. All subjects with previous spinal surgery or spinal deformities were excluded. The anteroposterior (AP) vertebral canal diameter was measured by two independent observers. Any associations between level-specific vertebral canal diameter and subject body habitus were analysed with non-parametric tests. Three or more stenotic levels, equivalent to a composite score of 3 or more, were considered as multilevel DSS. The median values of these subjects' AP canal diameters were used to construct the multilevel DSS values. Receiver operating characteristic analysis was utilized to determine the ability of these cut-off values to screen for DSS by presenting their area under curve, sensitivity and specificity.
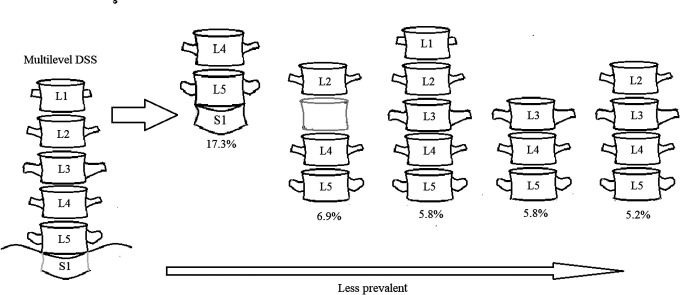
Subject body habitus was poorly correlated with AP vertebral canal diameter. Multilevel DSS was identified as L1<19 mm, L2<19 mm, L3<18 mm, L4<18 mm, L5<18 mm, S1<16 mm with 81%-96% sensitivity and 72%-91% specificity. The prevalence of multilevel DSS in this cohort was 7.3%.
Utilizing a large homogeneous cohort, the prevalence of multilevel DSS is determined. Our cut-offs provide high diagnostic accuracy. Patients with multiple levels that fulfil these criteria may be at-risk of spinal canal compressions at multiple sites.
III.
横断面研究。
使用综合评分模型定义多级腰椎发育性椎管狭窄(DSS)并确定其患病率。
这是一项对2385名公开招募的腰骶部(L1-S1)MRI受试者的队列研究。所有既往有脊柱手术或脊柱畸形的受试者均被排除。由两名独立观察者测量前后位(AP)椎管直径。采用非参数检验分析特定节段椎管直径与受试者身体形态之间的任何关联。三个或更多狭窄节段,相当于综合评分为3或更高,被视为多级DSS。这些受试者AP椎管直径的中位数用于构建多级DSS值。利用受试者工作特征分析,通过呈现曲线下面积、敏感性和特异性来确定这些临界值筛查DSS的能力。
受试者身体形态与AP椎管直径相关性较差。多级DSS被确定为L1<19mm,L2<19mm,L3<18mm,L4<18mm,L5<18mm,S1<16mm,敏感性为81%-96%,特异性为72%-91%。该队列中多级DSS的患病率为7.3%。
利用一个大型同质队列,确定了多级DSS的患病率。我们的临界值提供了较高的诊断准确性。符合这些标准的多个节段的患者可能存在多个部位椎管受压的风险。
III。