Immunology Division, The Walter and Eliza Hall Institute, Parkville, VIC, Australia.
Department of Medical Biology, University of Melbourne, Parkville, VIC, Australia.
BMC Med. 2020 Nov 26;18(1):362. doi: 10.1186/s12916-020-01828-y.
Patients with coeliac disease (CD) commonly report a variety of adverse symptoms to gluten, but descriptions of the symptomatic response in the literature may have been confounded by the presence of food components such as fermentable carbohydrates (FODMAPs) causing symptoms of irritable bowel syndrome independent of gluten. In recent unmasked and masked low FODMAP gluten challenge studies in small groups of treated CD patients, nausea and vomiting were shown to be the key symptoms associated with serum interleukin (IL)-2 release. Our objective was to utilise a large and diverse cohort of people with CD undertaking a standardised gluten food challenge to characterise the demographic, genetic and clinical factors influencing the severity and timing of acute gluten reactions and IL-2 production.
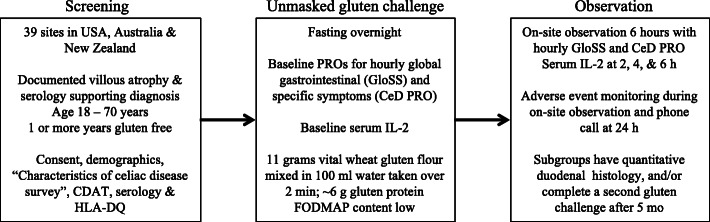
A total of 295 adults treated for CD were observed for 6 h after an unmasked food challenge consisting of 10 g vital wheat gluten (low in FODMAPs) in 100 ml water. Assessments included patient-reported outcomes, serum IL-2 and adverse events. Responses were analysed according to patient characteristics, HLA-DQ genotype, duodenal histology and response to a second gluten challenge.
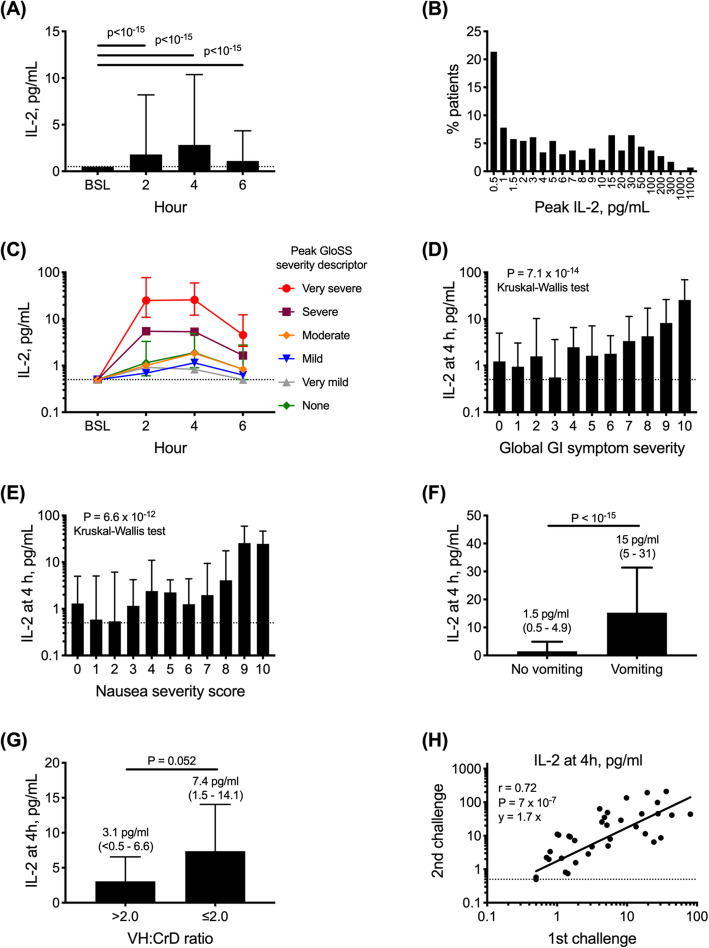
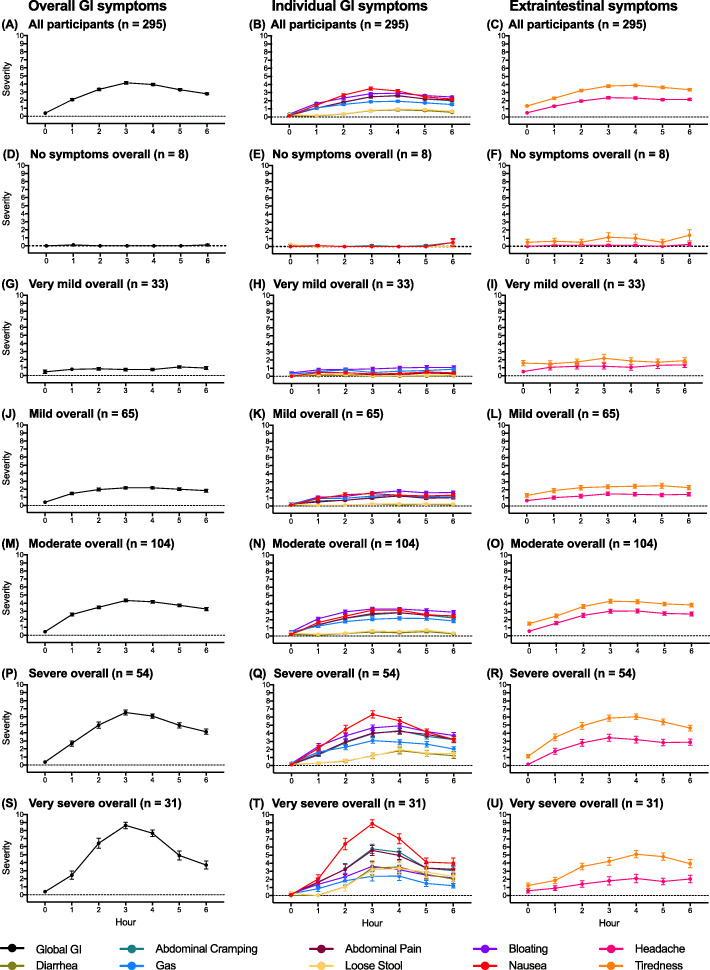
Peak symptom severity was at 3 h (median severity 5/10). Peak IL-2 was at 4 h (median 4 pg/ml, range undetectable to 1028 pg/ml). Older age, older age at diagnosis, HLA-DQ2.5 positivity and homozygosity for HLA-DQB1*02 were each significantly associated with IL-2 elevations after gluten. Patients positive for HLA-DQ2.5, DQ8, DQ2.2 or DQ7 showed elevated IL-2 after gluten. Patient factors were not significantly associated with severity of digestive symptoms, but symptoms were correlated to one another and serum IL-2. Gluten challenge after 5 months caused more vomiting and higher IL-2 levels, but responses correlated with the first.
Gluten-induced symptoms and cytokine release is common in adults with treated CD. Age, genetics and previous response to gluten predict these acute reactions to gluten challenge. Structured symptom assessment and serum IL-2 after standardised gluten challenge may inform on patient diagnosis, the role of gluten in symptomatology and the need for adjunctive treatment.
ClinicalTrials.gov , NCT03644069 Registered 21 May 2018.
乳糜泻(CD)患者常报告对麸质产生多种不良反应,但文献中对症状反应的描述可能因存在可发酵碳水化合物(FODMAPs)等食物成分而受到干扰,这些成分可引起与麸质无关的肠易激综合征症状。在最近针对少数接受治疗的 CD 患者进行的未掩蔽和掩蔽的低 FODMAP 麸质挑战研究中,恶心和呕吐被证明是与血清白细胞介素(IL)-2 释放相关的关键症状。我们的目的是利用大量不同的 CD 患者进行标准化的麸质食物挑战,以描述影响急性麸质反应和 IL-2 产生严重程度和时间的人口统计学、遗传和临床因素。
共有 295 名接受 CD 治疗的成年人在接受未掩蔽的食物挑战后 6 小时内接受观察,该挑战包含 100ml 水中的 10g 活力小麦麸质(低 FODMAPs)。评估包括患者报告的结果、血清 IL-2 和不良事件。根据患者特征、HLA-DQ 基因型、十二指肠组织学和对第二次麸质挑战的反应来分析反应。
峰值症状严重程度为 3 小时(中位数严重程度 5/10)。峰值 IL-2 为 4 小时(中位数 4pg/ml,范围不可检测到 1028pg/ml)。年龄较大、诊断时年龄较大、HLA-DQ2.5 阳性和 HLA-DQB1*02 纯合性与麸质后 IL-2 升高显著相关。HLA-DQ2.5、DQ8、DQ2.2 或 DQ7 阳性的患者在食用麸质后 IL-2 升高。患者因素与消化症状的严重程度无显著相关性,但症状相互关联且与血清 IL-2 相关。5 个月后进行的麸质挑战引起更多呕吐和更高的 IL-2 水平,但反应与第一次相关。
接受治疗的 CD 成人中,麸质诱导的症状和细胞因子释放很常见。年龄、遗传和以前对麸质的反应可预测这些对麸质挑战的急性反应。标准化麸质挑战后的结构化症状评估和血清 IL-2 可能有助于患者诊断、麸质在症状学中的作用以及辅助治疗的需要。
ClinicalTrials.gov,NCT03644069 于 2018 年 5 月 21 日注册。