Critical Care Research Group, Southampton National Institute of Health Research, Biomedical Research Centre, University Hospital Southampton, Southampton, UK; Integrative Physiology and Critical Illness Group, Clinical and Experimental Sciences, Faculty of Medicine, University of Southampton, Southampton, UK.
University of Plymouth, Plymouth Science Park, Plymouth, UK; Intensive Care Unit, Royal Free Hospital, London, UK.
Br J Anaesth. 2021 Mar;126(3):622-632. doi: 10.1016/j.bja.2020.09.050. Epub 2020 Nov 24.
The fraction of inspired oxygen (FiO) administered during general anaesthesia varies widely despite international recommendations to administer FiO 0.8 to all anaesthetised patients to reduce surgical site infections (SSIs). Anaesthetists remain concerned that high FiO administration intraoperatively may increase harm, possibly through increased oxidative damage and inflammation, resulting in more complications and worse outcomes. In previous systematic reviews associations between FiO and SSIs have been inconsistent, but none have examined how FiO affects perioperative oxidative stress. We aimed to address this uncertainty by reviewing the available literature.
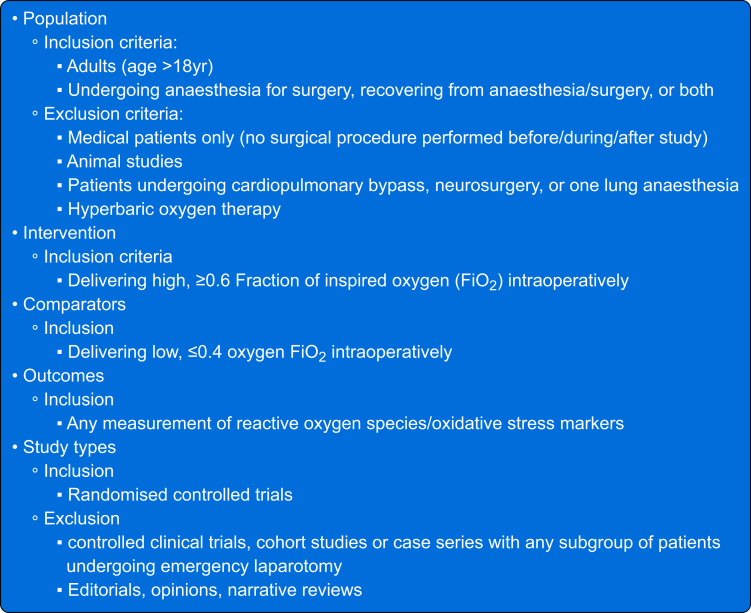
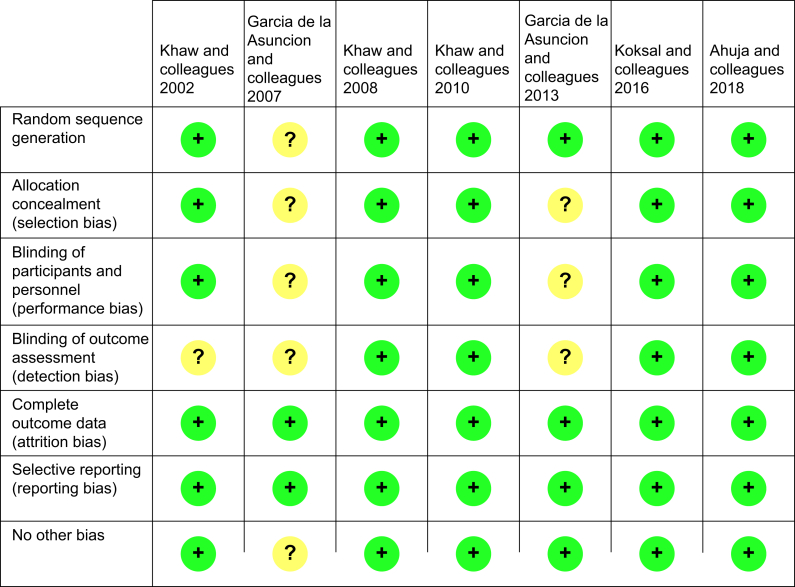
EMBASE, MEDLINE, and Cochrane databases were searched from inception to March 9, 2020 for RCTs comparing higher with lower perioperative FiO and quantifying oxidative stress in adults undergoing noncardiac surgery. Candidate studies were independently screened by two reviewers and references hand-searched. Methodological quality was assessed using the Cochrane Collaboration Risk of Bias tool.
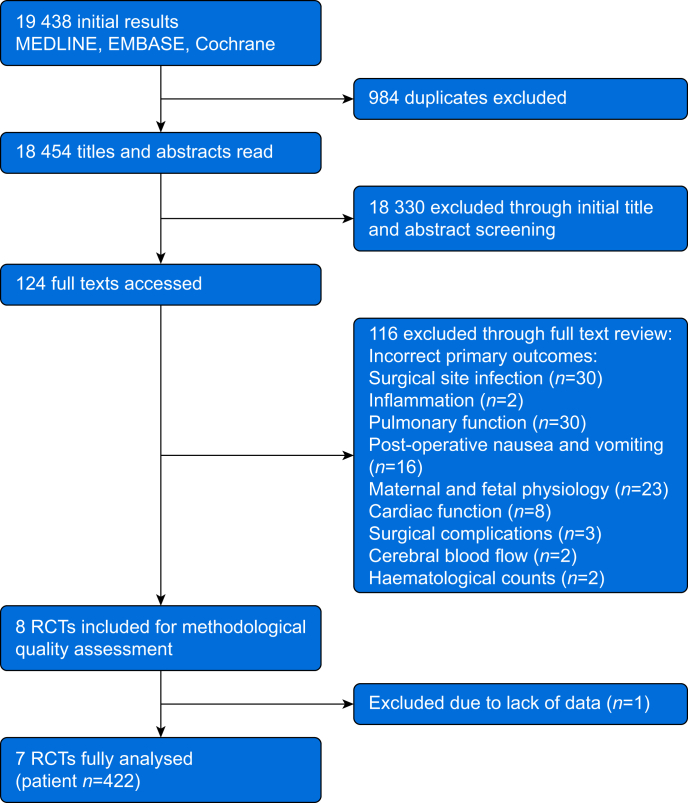
From 19 438 initial results, seven trials (n=422) were included. Four studies reported markers of oxidative stress during Caesarean section (n=328) and three reported oxidative stress during elective colon surgery (n=94). Risk of bias was low (four studies) to moderate (three studies). Pooled results suggested high FiO was associated with greater malondialdehyde, protein-carbonyl concentrations and reduced xanthine oxidase concentrations, together with reduced antioxidant markers such as superoxide dismutase and total sulfhydryl levels although total antioxidant status was unchanged.
Higher FiO may be associated with elevated oxidative stress during surgery. However, limited studies have specifically reported biomarkers of oxidation. Given the current clinical controversy concerning perioperative oxygen therapy, further research is urgently needed in this area.
尽管国际建议在所有接受全身麻醉的患者中给予 0.8FiO 以降低手术部位感染(SSI),但在全身麻醉期间给予的吸入氧分数(FiO)差异很大。麻醉师仍然担心术中高 FiO 给药可能会增加伤害,可能是通过增加氧化损伤和炎症,导致更多的并发症和更差的结果。在之前的系统评价中,FiO 与 SSI 之间的关联一直不一致,但没有一项研究检查 FiO 如何影响围手术期氧化应激。我们旨在通过审查现有文献来解决这一不确定性。
从 2020 年 3 月 9 日起,在 EMBASE、MEDLINE 和 Cochrane 数据库中搜索了比较高与低围手术期 FiO 并量化非心脏手术成人氧化应激的 RCT。两名评审员独立筛选候选研究,并手动搜索参考文献。使用 Cochrane 协作风险偏倚工具评估方法学质量。
从 19438 个初始结果中,纳入了 7 项试验(n=422)。四项研究报告了剖宫产术中(n=328)的氧化应激标志物,三项研究报告了择期结肠手术中的氧化应激标志物(n=94)。风险偏倚低(四项研究)至中度(三项研究)。汇总结果表明,高 FiO 与更高的丙二醛、蛋白羰基浓度和降低的黄嘌呤氧化酶浓度相关,同时降低了超氧化物歧化酶和总巯基水平等抗氧化标志物,但总抗氧化状态不变。
较高的 FiO 可能与手术期间氧化应激增加有关。然而,有限的研究专门报告了氧化的生物标志物。鉴于目前围手术期氧疗的临床争议,迫切需要在这一领域进行进一步研究。