Department of Psychology, Temple University, Weiss Hall, 1701 N. 13th St., Philadelphia, PA 19122, USA.
Department of Psychology, University of Amsterdam, Nieuwe Achtergracht 129-B, 1018 WT Amsterdam, The Netherlands.
Brain Behav Immun. 2021 Mar;93:35-42. doi: 10.1016/j.bbi.2020.12.005. Epub 2020 Dec 9.
There has been increasing interest in classifying inflammatory phenotypes of depression. Most investigations into inflammatory phenotypes only have tested whether elevated inflammation is associated with elevated levels of depression symptoms, or risk for a diagnosis. This study expanded the definition of phenotype to include the structure of depression symptoms as a function of inflammation.
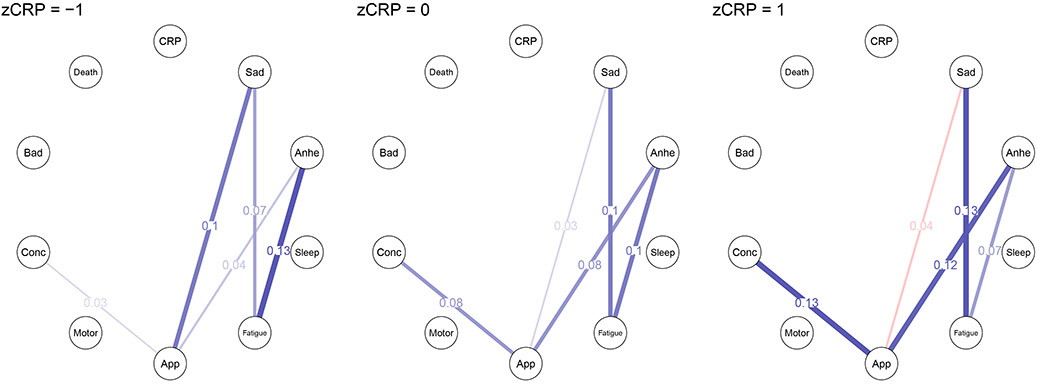
Network models of depression symptoms were estimated in a sample of 4157 adults (mean age = 47.6, 51% female) from the 2015-2016 National Health and Nutrition Examination Survey (NHANES). Analyses included comparisons of networks between those with elevated (C-reactive protein (CRP) values ≥ 3.0 mg/L; N = 1696) and non-elevated CRP (N = 2841) as well as moderated network models with CRP group status and raw CRP values moderating the associations between depression symptoms.
Differences emerged at all levels of analysis (global, symptom-specific, symptom-symptom associations). Specifically, the elevated CRP group had greater symptom connectivity (stronger total associations between symptoms). Further, difficulty concentrating and psychomotor difficulties had higher expected influence (concordance with other symptoms) in the elevated CRP group. Finally, there was evidence that several symptom-symptom associations were moderated by CRP.
This study provides consistent evidence that the structure of depression symptoms varies as a function of CRP levels. Greater symptom connectivity might contribute to why elevated CRP is associated with treatment-resistant depression. Additionally, differences in symptom structure might highlight different maintenance mechanisms and treatment targets for individuals with compared to those without elevated CRP. Finally, differences in symptom structure as a function of CRP highlight a potential misalignment of standard depression measures (the structure of which are evaluated on groups unselected for CRP levels) and the presentation of depression symptoms in those with elevated CRP.
人们对抑郁症的炎症表型分类越来越感兴趣。大多数炎症表型的研究仅测试了炎症水平升高是否与抑郁症状升高或诊断风险相关。本研究扩展了表型的定义,将抑郁症状的结构作为炎症的一个功能包含在内。
在来自 2015-2016 年全国健康和营养检查调查(NHANES)的 4157 名成年人(平均年龄为 47.6 岁,51%为女性)样本中,估计了抑郁症状的网络模型。分析包括对 CRP 值升高(C-反应蛋白(CRP)值≥3.0mg/L;N=1696)和 CRP 值不升高(N=2841)人群网络之间的比较,以及 CRP 组状态和 CRP 值的调节网络模型与抑郁症状之间的关联。
在所有分析水平(全局、症状特异性、症状-症状关联)上都出现了差异。具体来说,CRP 升高组的症状连接性更强(症状之间的总关联更强)。此外,在 CRP 升高组中,注意力不集中和精神运动困难的预期影响(与其他症状的一致性)更高。最后,有证据表明,几个症状-症状的关联受 CRP 调节。
本研究提供了一致的证据表明,抑郁症状的结构随着 CRP 水平的变化而变化。更强的症状连接性可能是 CRP 升高与治疗抵抗性抑郁症相关的原因之一。此外,症状结构的差异可能突出了与 CRP 升高的个体相比,没有 CRP 升高的个体的不同维持机制和治疗靶点。最后,CRP 作为一个函数的症状结构差异突出了标准抑郁测量(其结构在未选择 CRP 水平的人群中进行评估)与 CRP 升高者的抑郁症状表现之间的潜在不匹配。