Renal Division, Department of Medicine, Peking University First Hospital, Beijing, 100034, People's Republic of China.
Institute of Nephrology, Peking University, Beijing, 100034, People's Republic of China.
BMC Nephrol. 2021 Jan 6;22(1):6. doi: 10.1186/s12882-020-02204-x.
Multiple myeloma (MM) is a plasma-cell derived hematologic malignant disease. The malignant proliferating plasma cells secrete massive monoclonal immunoglobulins which lead to various pathologic types of renal injury. Myeloma cast nephropathy (MCN) is the most common histopathologic lesion with the worst renal prognosis. Rarely, the free light chains in the protein casts can form amyloid fibrils. Here, we reported two rare cases of MCN with diffuse amyloid casts.
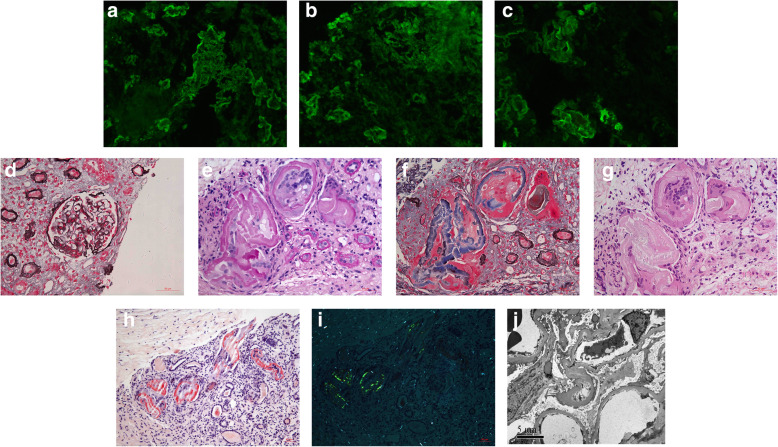
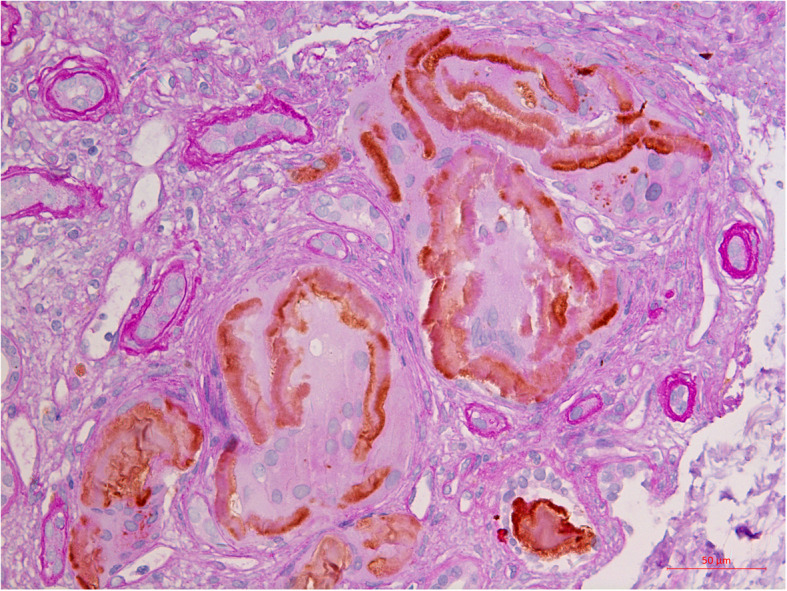
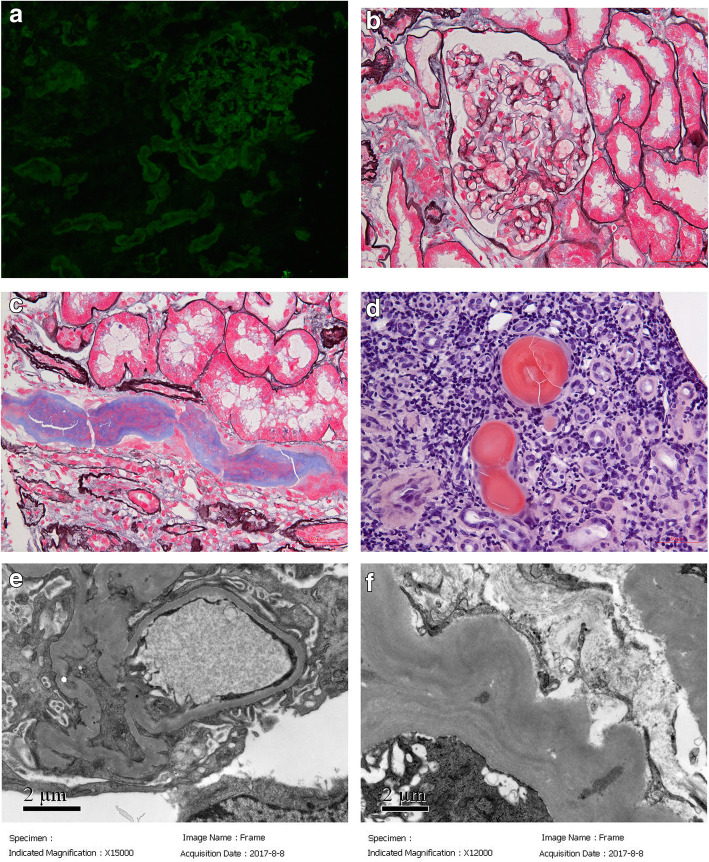
Case 1: A 54-year-old Chinese man presented with a 4-year history of multiple myeloma, proteinuria and hematuria. He had monoclonal IgAλ plus free λ spike in both serum and urine. He had been on chemotherapy for 4 years and maintained normal serum creatinine until 11 months ago. Then, his renal function deteriorated and he went on hemodialysis 4 months before admission. Renal biopsy showed diffuse amyloid casts in the tubular lumens, without any obvious amyloid deposits in other kidney compartments or signs of extra-renal amyloidosis. The amyloid fibrils formed around mononuclear cells which were CD68 negative. According to the morphology and location, these mononuclear cells were considered as tubular epithelial cells. The patient was maintained on chemotherapy and hemodialysis. He died 8 months after renal biopsy. Case 2: A 58-year-old Chinese man presented with a one-and-a-half-year history of proteinuria and slowly rising serum creatinine. He had monoclonal IgDλ spike in both serum and urine. Amyloid casts were observed in the tubular lumens and mononuclear cells could be identified in the center of some casts. There were no amyloid deposits in other kidney compartments and no sign of systemic amyloidosis. The patient also had fine granular deposits along the tubular basement membrane with λ linear staining along tubular basement membrane suggesting light chain deposition disease. He was treated with bortezomib-based chemotherapy followed by lenalidomide-based chemotherapy and achieved very good partial remission (VGPR). After 27 months of follow-up, the patient still showed no signs of systemic amyloidosis.
These 2 cases of MCN with diffuse amyloid casts have different histopathologic characteristics from the usual myeloma casts and tubular epithelial cells might play important roles in the pathogenesis.
多发性骨髓瘤(MM)是一种浆细胞来源的血液恶性肿瘤。恶性增殖的浆细胞分泌大量单克隆免疫球蛋白,导致各种类型的肾损伤。骨髓瘤管型肾病(MCN)是最常见的组织病理学病变,也是预后最差的病变。罕见情况下,蛋白管型中的游离轻链可形成淀粉样纤维。在此,我们报告两例罕见的弥漫性淀粉样纤维管型的 MCN 病例。
病例 1:一名 54 岁的中国男性,患有多发性骨髓瘤 4 年,有蛋白尿和血尿。他的血清和尿液中均存在单克隆 IgAλ 加游离 λ 峰。他已经接受了 4 年的化疗,血清肌酐一直正常,直到 11 个月前。随后,他的肾功能恶化,在入院前 4 个月开始接受血液透析。肾活检显示管状腔中有弥漫性淀粉样纤维管型,其他肾脏部位无明显淀粉样沉积物或肾脏外淀粉样变性迹象。淀粉样纤维围绕单核细胞形成,CD68 阴性。根据形态和位置,这些单核细胞被认为是肾小管上皮细胞。患者继续接受化疗和血液透析。肾活检后 8 个月死亡。病例 2:一名 58 岁的中国男性,患有蛋白尿和血清肌酐缓慢升高 1 年半。他的血清和尿液中均存在单克隆 IgDλ 峰。管状腔中观察到淀粉样纤维管型,一些管型的中心可识别出单核细胞。其他肾脏部位无淀粉样沉积物,无系统性淀粉样变性迹象。患者还沿肾小管基底膜有细颗粒沉积,λ 线性沿肾小管基底膜染色提示轻链沉积病。他接受硼替佐米为基础的化疗,随后接受来那度胺为基础的化疗,达到非常好的部分缓解(VGPR)。随访 27 个月后,患者仍无系统性淀粉样变性迹象。
这两例弥漫性淀粉样纤维管型的 MCN 具有与常见骨髓瘤管型不同的组织病理学特征,肾小管上皮细胞可能在发病机制中起重要作用。