Hadaegh Farzad, Asgari Samaneh, Moosaie Fatemeh, Orangi Meysam, Sarvghadi Farzaneh, Khalili Davood, Azizi Fereidoun
Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Islamic Republic of Iran.
Tehran University of Medical Sciences, Tehran, Iran.
J Transl Med. 2021 Jan 6;19(1):25. doi: 10.1186/s12967-020-02686-1.
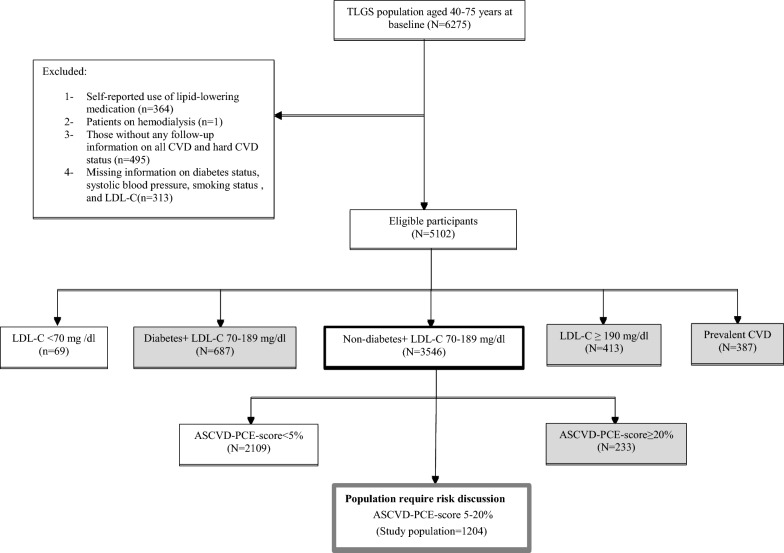
In 2013 American College of Cardiology and the American Heart Association released a guideline on the management of atherosclerotic cardiovascular disease (ASCVD) including a composite of death from CVD, non-fatal myocardial infarction, or non-fatal stroke (hard CVD). This guideline recommended a risk score that was calculated using pooled cohort equations (ASCVD-PCE). The guideline was updated in 2018/2019 and further risk discussion was suggested for deciding whether to continue or initiate statin therapy among non-diabetic individuals with ASCVD-PCE score ranged 5-20%. They recommended a risk discussion with considering risk enhancing factors (ASCVD-REFs) including family history of premature CVD, chronic kidney disease, triglycerides ≥ 175 mg/dl, low-density lipoprotein cholesterol (LDL-C) ≥ 160 mg/dl, metabolic syndrome (Mets), and for women premature menopause, and hypertensive disorders of pregnancy (HDP). In the current study, we aimed to examine the predictability of recommended ASCVD-REFs on incident hard CVD in non-diabetic individuals with LDL-C 70-189 mg/dl, with ASCVD-PCE risk 5-20% during 10 and 15-year follow-up.
Among a total of 3546 non-diabetic individuals aged 40-75 years, after excluding those with ASCVD-PCE score < 5% and ≥ 20% (n = 2342), 1204 individuals (women = 332) were included. The univariable and multivariable (further adjusted for ASCVD-PCE) Cox regression analysis were used to evaluate the association of each potential ASCVD-REFs with hard CVD. Additionnaly, the role of different components of Mets and a history of gestational diabetes (GDM)/macrosomia was also examined. The predictive ability of each significant ASCVD-REFs, then was evaluated by the discrimination accuracy and risk reclassification index.
During the 10-year follow-up, 73 hard CVD events occurred. Although in univariable analysis, high blood pressure (BP) component of Mets, GDM/macrosomia, and HDP remained as significant ASCVD-REFs, in the multivariable analysis, only the history of HDP (5.35 (1.22-23.38)) and GDM/macrosomia (3.18 (1.05-9.65)) showed independent risks. During the 15-year follow-up, Mets (1.47 (1.05-2.06)) and its components of high waist circumference (1.40 (1.0-1.95)) and high BP (1.52 (1.07-2.15)) significantly increased the risk. These ASCVD-REFs did not improve discrimination or predictive ability.
In a decade follow-up, only conditions specific for women and in longer follow-up, the presence of Mets perse, and its components of high WC and high BP were shown as significant ASCVD-REFs.
2013年,美国心脏病学会和美国心脏协会发布了一份关于动脉粥样硬化性心血管疾病(ASCVD)管理的指南,其中包括心血管疾病死亡、非致死性心肌梗死或非致死性中风(严重心血管疾病)的综合指标。该指南推荐了一种使用合并队列方程(ASCVD-PCE)计算的风险评分。该指南在2018/2019年进行了更新,并建议在ASCVD-PCE评分在5%-20%的非糖尿病个体中,就是否继续或启动他汀类药物治疗进行进一步的风险讨论。他们建议在考虑风险增强因素(ASCVD-REFs)的情况下进行风险讨论,这些因素包括早发性心血管疾病家族史、慢性肾病、甘油三酯≥175mg/dl、低密度脂蛋白胆固醇(LDL-C)≥160mg/dl、代谢综合征(Mets),以及女性的过早绝经和妊娠期高血压疾病(HDP)。在本研究中,我们旨在探讨推荐的ASCVD-REFs对LDL-C为70-189mg/dl、ASCVD-PCE风险为5%-20%的非糖尿病个体在10年和15年随访期间发生严重心血管疾病的预测能力。
在总共3546名年龄在40-75岁的非糖尿病个体中,排除ASCVD-PCE评分<5%和≥20%的个体(n=2342)后,纳入1204名个体(女性=332)。采用单变量和多变量(进一步根据ASCVD-PCE进行调整)Cox回归分析来评估每个潜在的ASCVD-REFs与严重心血管疾病的关联。此外,还研究了Mets不同组成部分以及妊娠期糖尿病(GDM)/巨大儿病史的作用。然后,通过辨别准确性和风险重新分类指数评估每个显著的ASCVD-REFs的预测能力。
在10年随访期间,发生了73例严重心血管疾病事件。虽然在单变量分析中,Mets中的高血压(BP)组成部分、GDM/巨大儿和HDP仍然是显著的ASCVD-REFs,但在多变量分析中,只有HDP病史(5.35(1.22-23.38))和GDM/巨大儿(3.18(