Yu Marc Gregory, Blanquisco Louren, Ańonuevo-Cruz Ma Cecille
Section of Endocrinology, Diabetes, and Metabolism, Department of Medicine, Philippine General Hospital.
J ASEAN Fed Endocr Soc. 2017;32(1):20-26. doi: 10.15605/jafes.032.01.04. Epub 2017 Apr 11.
To evaluate the safety and efficacy of heparinoid supplementation on all-cause mortality and disease progression in diabetic kidney disease (DKD).
Trials evaluating heparinoid supplementation in DKD were included. Two authors performed a literature search with eligible studies undergoing validity screen, data extraction, and statistical analysis. Results were calculated using the Mantel-Haenszel odds ratio for dichotomous variables and the inverse variance method for continuous variables, and pooled using a random or fixed effects model depending on heterogeneity.
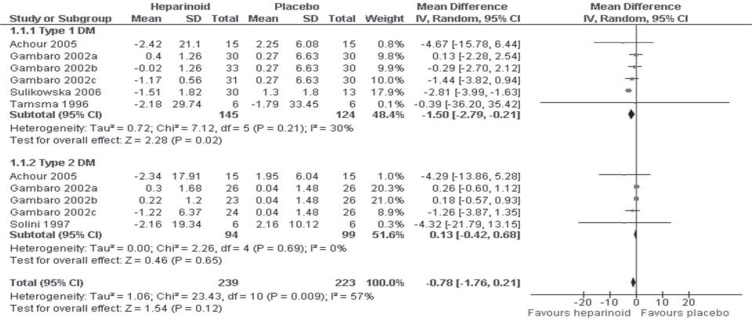
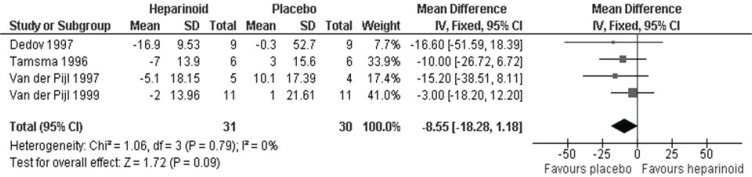
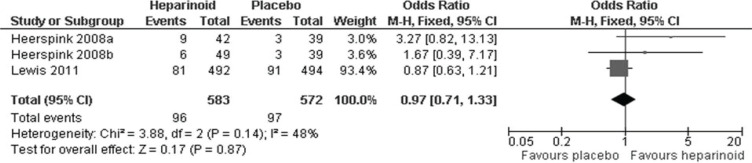
Twelve trials were included in the analysis. Eight involved sulodexide while two each involved low molecular weight heparin and danaparoid. We found no statistically significant difference between the heparinoid and placebo groups for all-cause mortality (95% CI, HR 0.79 [0.41, 1.53], p=0.49), number of patients reaching therapeutic success (95% CI, OR 0.97 [0.71, 1.33], p=0.87), serum creatinine (95% CI, MD 2.55 umol/L [-0.54, 5.65], p=0.11), and creatinine clearance (95% CI, MD -8.55 mg/min [-18.28, 1.18], p=0.09). We also found no statistically significant difference in urinary albumin excretion rate (UAER) between Type 2 heparinoid-treated DKD patients compared to placebo (95% CI, log transformed MD 0.13 mg/24h [-0.42, 0.68], p=0.65); however, a statistically significant UAER reduction was seen in Type 1 heparinoid-treated DKD patients compared to placebo (95% CI, log-transformed MD -1.5 mg/24h [-2.79, -0.21], p=0.02). This subgroup analysis was performed due to initial heterogeneity (I=57%).
Heparinoid supplementation was not associated with statistically significant changes in Type 2 DM patients. However, it may be associated with a statistically significant UAER reduction of approximately 31.62 mg/24 h as compared to placebo in Type 1 DM patients. Due to sparse data on hard clinical outcomes, larger studies are recommended.
评估补充类肝素对糖尿病肾病(DKD)全因死亡率和疾病进展的安全性及疗效。
纳入评估补充类肝素治疗DKD的试验。两位作者进行文献检索,对符合条件的研究进行效度筛选、数据提取和统计分析。二分类变量的结果采用Mantel-Haenszel比值比计算,连续变量采用逆方差法计算,并根据异质性采用随机或固定效应模型进行合并。
分析纳入12项试验。8项涉及舒洛地特,2项分别涉及低分子量肝素和达那肝素。我们发现,在全因死亡率方面,类肝素组与安慰剂组之间无统计学显著差异(95%CI,HR 0.79[0.41, 1.53],p = 0.49);在达到治疗成功的患者数量方面(95%CI,OR 0.97[0.71, 1.33],p = 0.87);在血清肌酐方面(95%CI,MD 2.55 μmol/L[-0.54, 5.65],p = 0.11);在肌酐清除率方面(95%CI,MD -8.55 mg/min[-18.28, 1.18],p = 0.09)。与安慰剂相比,我们还发现2型类肝素治疗的DKD患者尿白蛋白排泄率(UAER)无统计学显著差异(95%CI,对数转换MD 0.13 mg/24h[-0.42, 0.68],p = 0.65);然而,与安慰剂相比,1型类肝素治疗的DKD患者UAER有统计学显著降低(95%CI,对数转换MD -1.5 mg/24h[-2.79, -0.21],p = 0.02)。进行该亚组分析是由于初始存在异质性(I = 57%)。
补充类肝素与2型糖尿病患者的统计学显著变化无关。然而,与安慰剂相比,1型糖尿病患者补充类肝素可能与UAER统计学显著降低约31.62 mg/24 h有关。由于关于硬临床结局的数据稀少,建议开展更大规模的研究。