Department of Radiation Oncology, Government Medical College and Hospital, Chandigarh, India.
Department of Community Medicine and School of Public Health, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
JCO Glob Oncol. 2021 Jan;7:108-117. doi: 10.1200/GO.20.00288.
Glioblastoma multiforme (GBM) has poor outcomes following surgery and radiation. Adjuvant temozolamide along with radiation therapy has been shown to improve survival. In this paper, we evaluate the cost-effectiveness of concomitant temozolamide with radiation and maintenance temozolamide for 6 months of treatment for GBM in India.
We used a Markov model to evaluate the lifetime costs and consequences of treating GBM with radiation alone versus radiation with adjuvant temozolamide. The model was calibrated using the published evidence from European Organisation for Research and Treatment of Cancer-NCIC trial on progression-free survival and overall survival to estimate the life years (LYs) and quality-adjusted LYs (QALYs). Cost of treatment and management of complications were estimated using the data from the National Health System Cost Database and Indian studies. Future cost and consequences were discounted at 3%. Incremental cost per QALY gained with temozolamide was estimated to assess cost effectiveness.
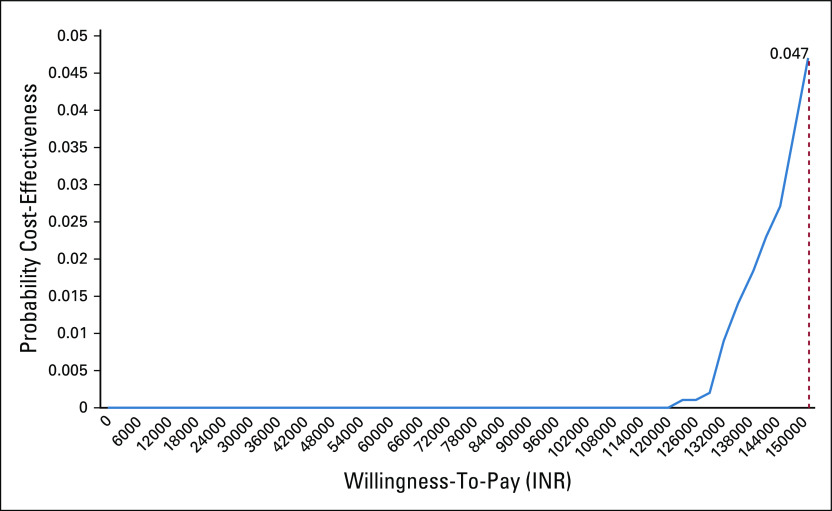
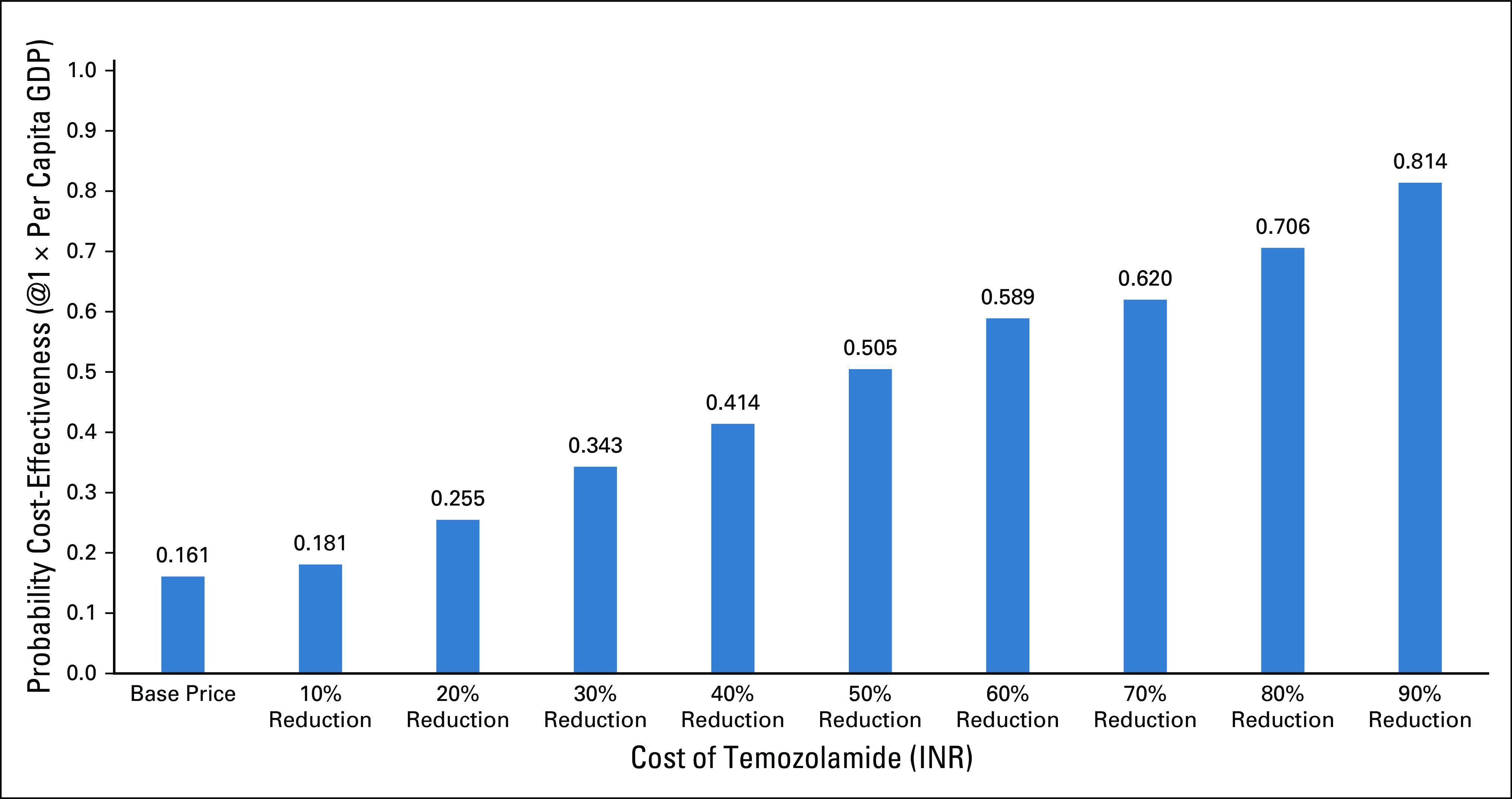
Temozolamide resulted in an increase of 0.59 (0.53-0.66) LY and 0.33 (0.29-0.40) QALY per person at an incremental cost of ₹75,120 in Indian national rupee (INR) (59,337-93,960). Overall, the use of temozolamide incurs an incremental cost of ₹212,020 INR (138,127-401,466) per QALY gained, which has a 4.7% probability to be cost-effective at 1-time per capita Gross Domestic Product (GDP) threshold. In case the current price of temozolamide could be decreased by 90%, the probability of its use for GBM being cost-effective increases to 80%.
Temozolamide is not cost-effective for treatment of patients with GBM in India. This evidence should be used while framing guidelines for treatment and price regulation.
胶质母细胞瘤(GBM)在手术后和放疗后预后较差。辅助替莫唑胺联合放疗已被证明可提高生存率。本文评估了替莫唑胺与放疗联合应用和 6 个月替莫唑胺维持治疗在印度治疗 GBM 的成本效益。
我们使用马尔可夫模型来评估单独放疗与放疗联合替莫唑胺辅助治疗 GBM 的终生成本和结果。该模型使用欧洲癌症研究与治疗组织-NCIC 试验的无进展生存期和总生存期的发表证据进行校准,以估计寿命年(LY)和质量调整寿命年(QALY)。使用国家卫生系统成本数据库和印度研究的数据来估计治疗和并发症管理的成本。未来的成本和结果以 3%的贴现率进行贴现。使用增量成本每获得一个 QALY 来评估成本效益。
替莫唑胺使每人的 LY 增加 0.59(0.53-0.66),QALY 增加 0.33(0.29-0.40),增量成本为 75120 印度卢比(INR)(59337-93960)。总体而言,使用替莫唑胺使每个 QALY 的增量成本为 212020 印度卢比(INR)(138127-401466),在人均国内生产总值(GDP)阈值为 1 次时,有 4.7%的可能性具有成本效益。如果替莫唑胺的当前价格能够降低 90%,则其用于治疗 GBM 的成本效益的可能性将增加到 80%。
替莫唑胺在印度治疗 GBM 患者的成本效益不高。在制定治疗和价格监管指南时,应考虑这一证据。