Department of Radiology, Duke University, 2424 Erwin Rd, Ste 302, Durham, NC 27705.
Department of Electrical and Computer Engineering, Duke University, Durham, NC.
AJR Am J Roentgenol. 2021 Mar;216(3):824-834. doi: 10.2214/AJR.19.22482. Epub 2021 Jan 21.
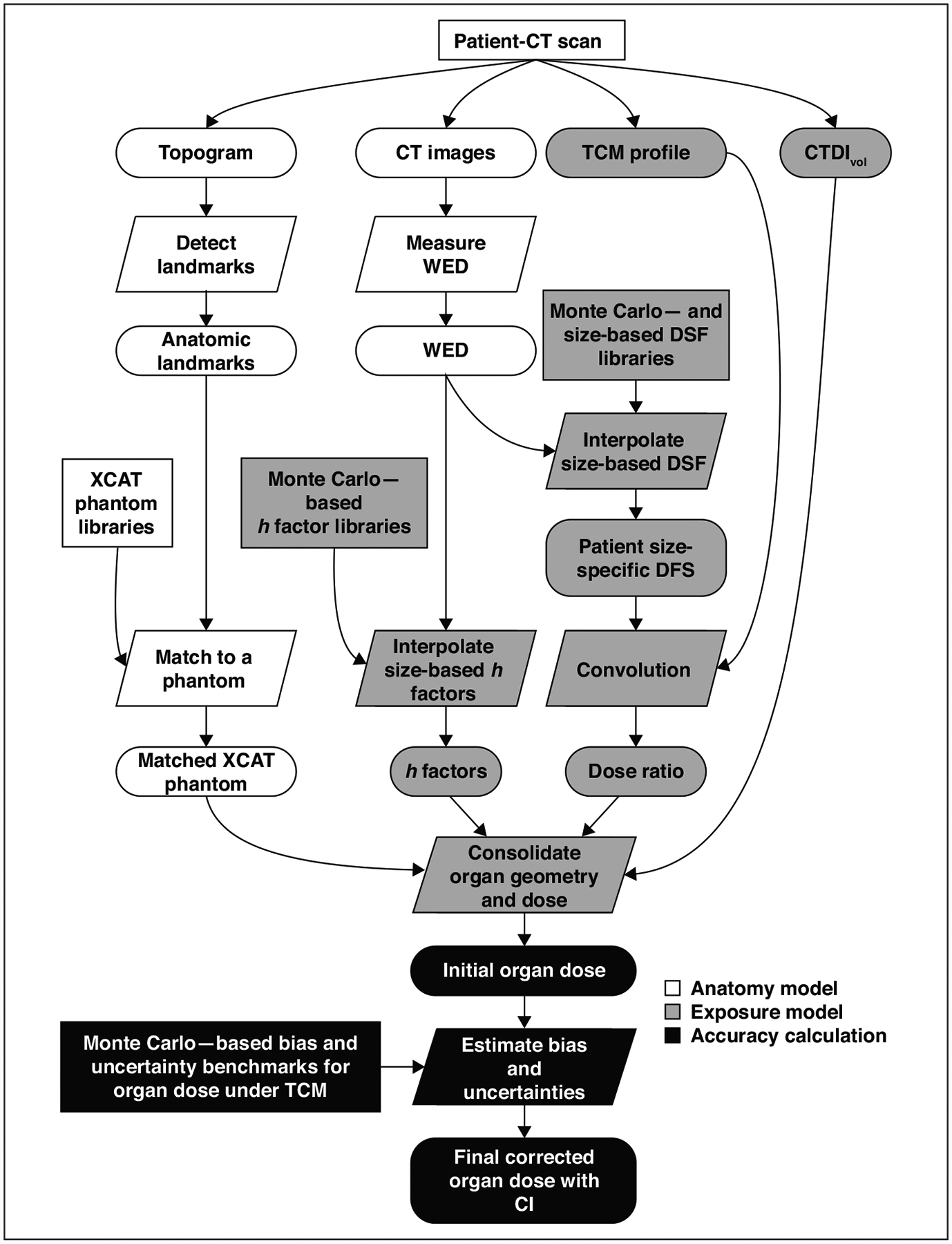
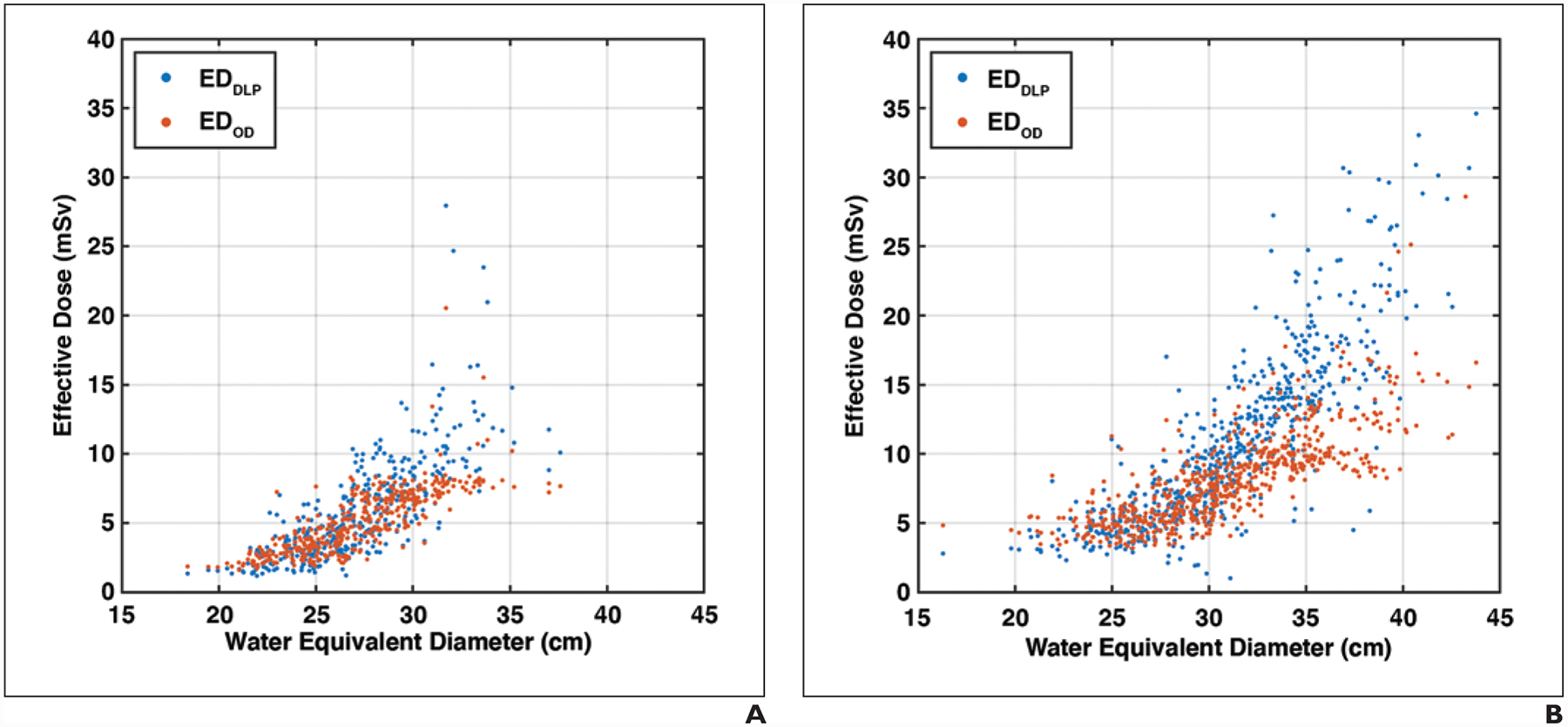
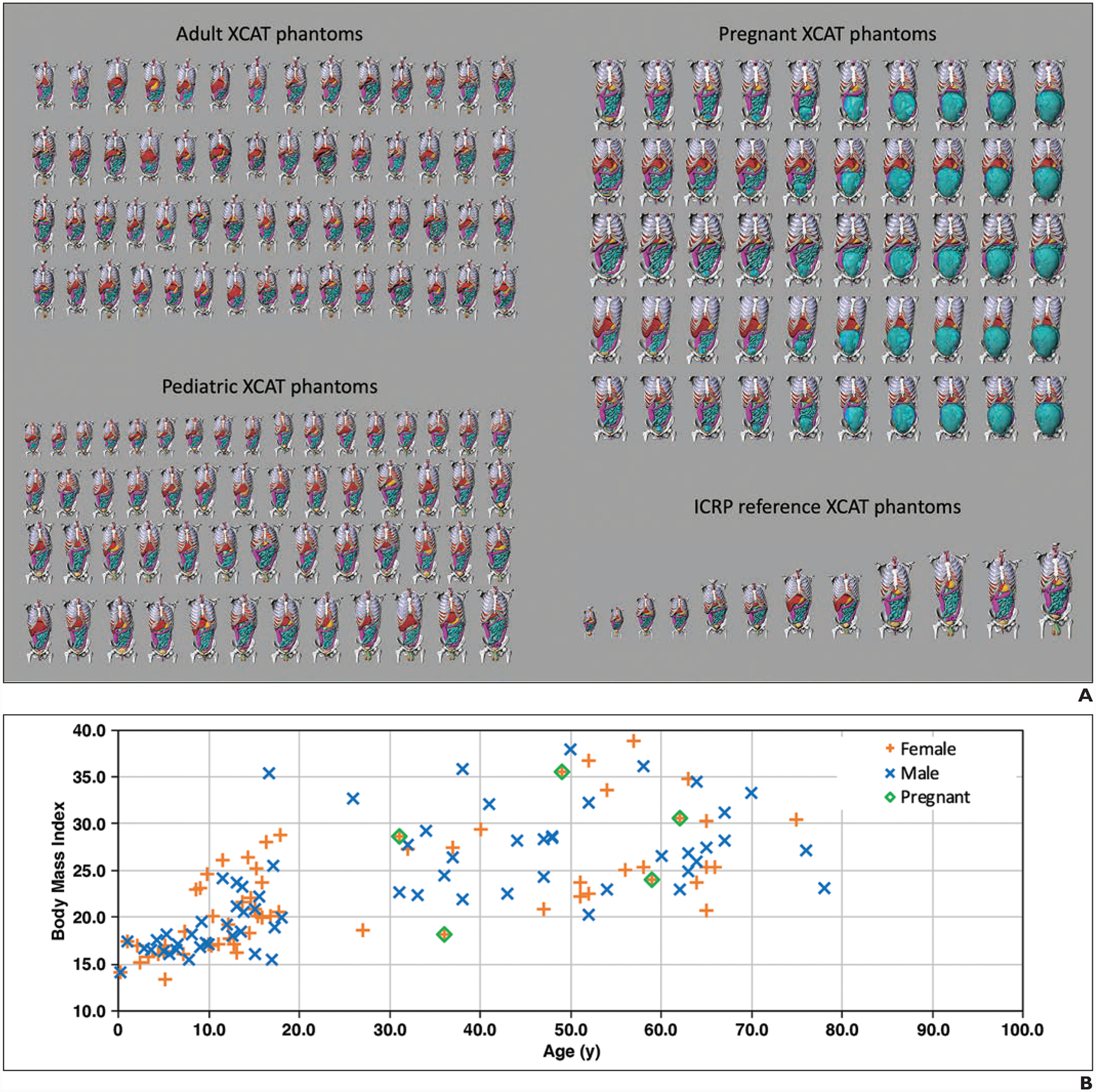
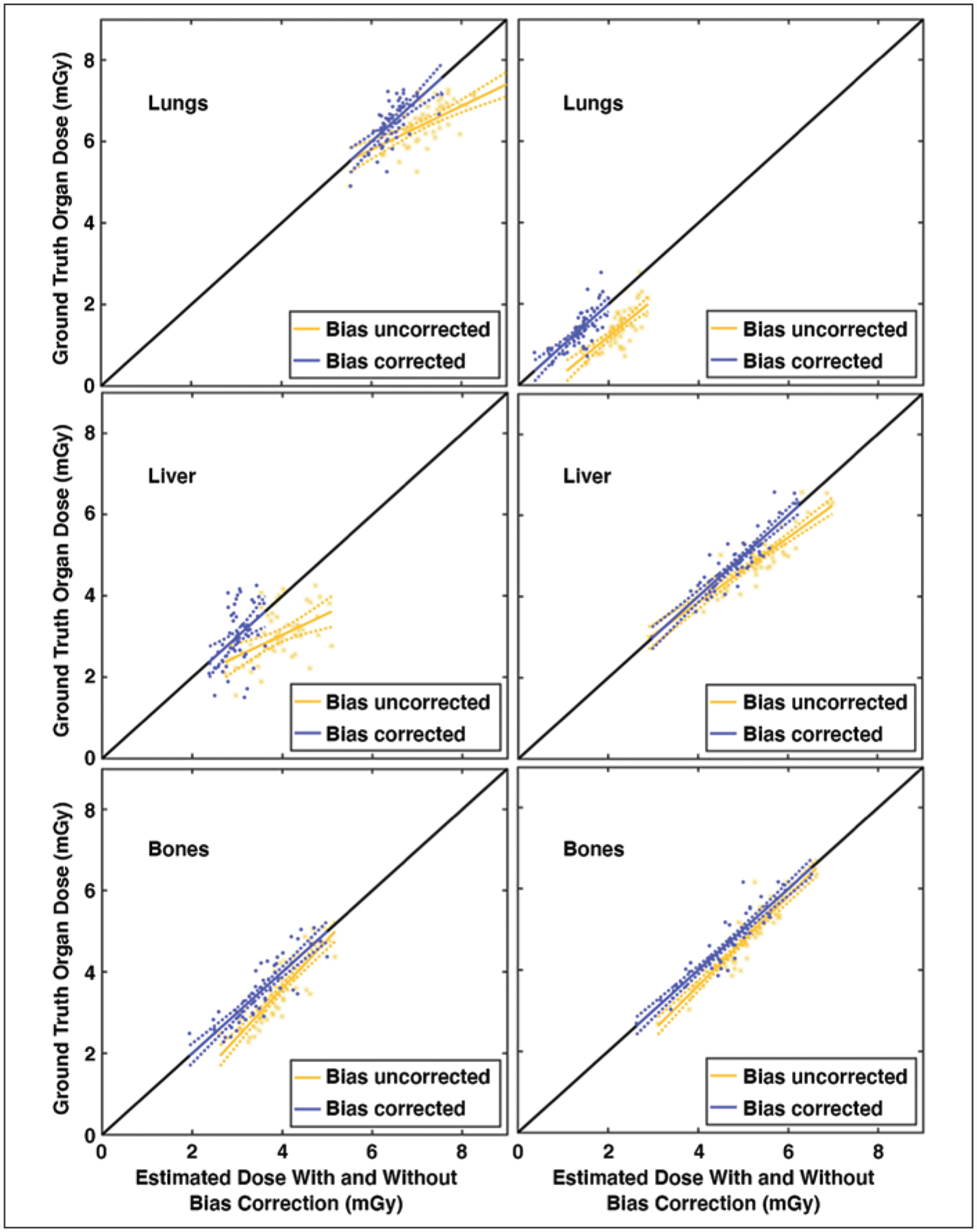
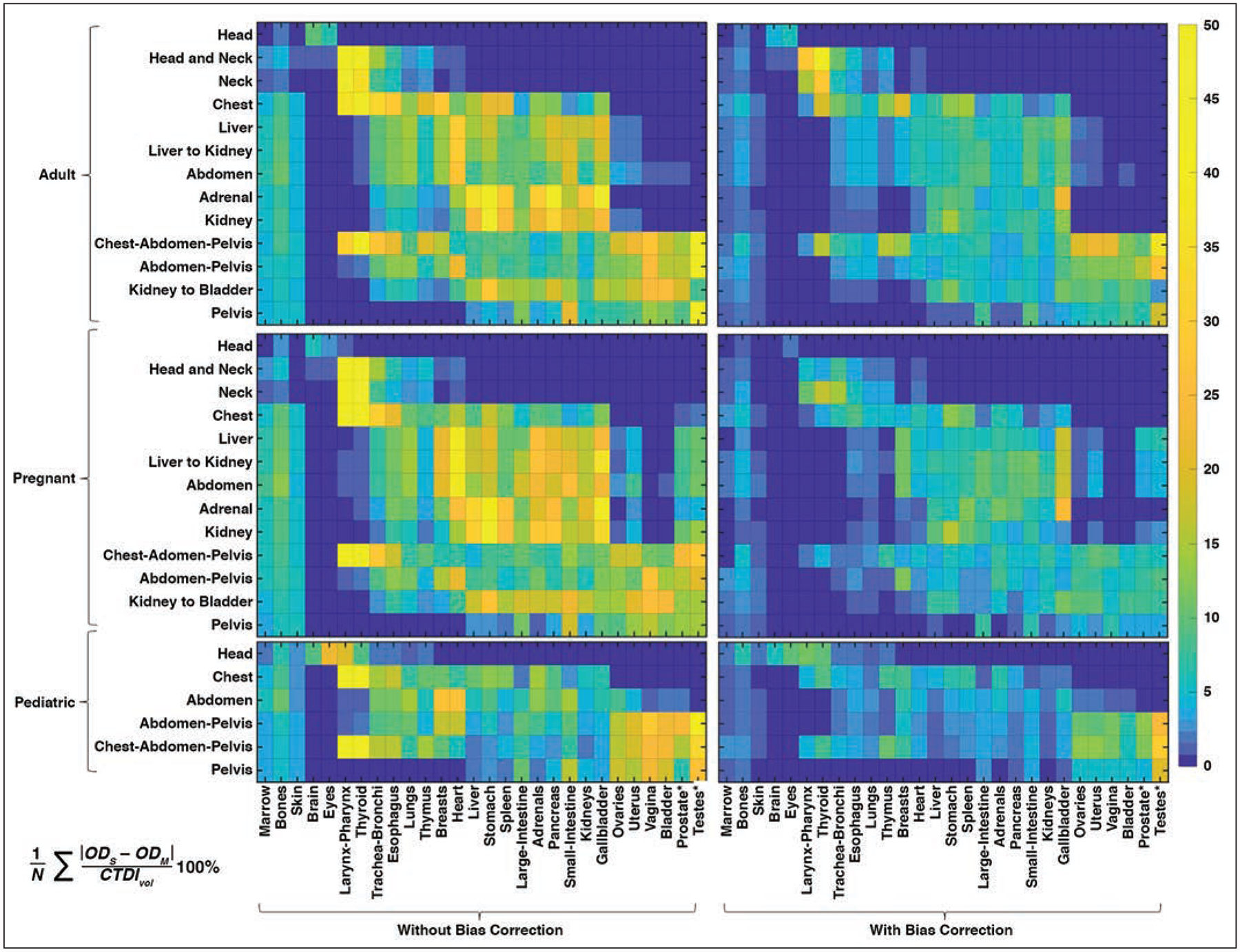
The purpose of this study is to comprehensively implement a patient-informed organ dose monitoring framework for clinical CT and compare the effective dose (ED) according to the patient-informed organ dose with ED according to the dose-length product (DLP) in 1048 patients. Organ doses for a given examination are computed by matching the topogram to a computational phantom from a library of anthropomorphic phantoms and scaling the fixed tube current dose coefficients by the examination volume CT dose index (CTDI) and the tube-current modulation using a previously validated convolution-based technique. In this study, the library was expanded to 58 adult, 56 pediatric, five pregnant, and 12 International Commission on Radiological Protection (ICRP) reference models, and the technique was extended to include multiple protocols, a bias correction, and uncertainty estimates. The method was implemented in a clinical monitoring system to estimate organ dose and organ dose-based ED for 647 abdomen-pelvis and 401 chest examinations, which were compared with DLP-based ED using a test. For the majority of the organs, the maximum errors in organ dose estimation were 18% and 8%, averaged across all protocols, without and with bias correction, respectively. For the patient examinations, DLP-based ED was significantly different from organ dose-based ED by as much as 190.9% and 234.7% for chest and abdomen-pelvis scans, respectively (mean, 9.0% and 24.3%). The differences were statistically significant ( < .001) and exhibited overestimation for larger-sized patients and underestimation for smaller-sized patients. A patient-informed organ dose estimation framework was comprehensively implemented applicable to clinical imaging of adult, pediatric, and pregnant patients. Compared with organ dose-based ED, DLP-based ED may overestimate effective dose for larger-sized patients and underestimate it for smaller-sized patients.
本研究旨在全面实施基于患者知情的临床 CT 器官剂量监测框架,并比较 1048 例患者中基于患者知情的器官剂量与基于剂量长度乘积(DLP)的有效剂量(ED)。通过将体层摄影与来自人体模型库的计算体模匹配,计算特定检查的器官剂量,并通过检查体积 CT 剂量指数(CTDI)和管电流调制对固定管电流剂量系数进行缩放,使用以前验证的基于卷积的技术。在本研究中,该库扩展到 58 个成人、56 个儿科、5 个孕妇和 12 个国际辐射防护委员会(ICRP)参考模型,并将该技术扩展到包括多个协议、偏置校正和不确定度估计。该方法在临床监测系统中实施,以估计 647 例腹部-骨盆和 401 例胸部检查的器官剂量和基于器官剂量的 ED,并使用 t 检验与基于 DLP 的 ED 进行比较。对于大多数器官,在没有和有偏置校正的情况下,跨所有协议平均,器官剂量估计的最大误差分别为 18%和 8%。对于患者检查,基于 DLP 的 ED 与基于器官剂量的 ED 差异显著,胸部和腹部-骨盆扫描分别高达 190.9%和 234.7%(平均 9.0%和 24.3%)。差异具有统计学意义( <.001),并且对于较大体型的患者高估,对于较小体型的患者低估。已经全面实施了基于患者知情的器官剂量估计框架,适用于成人、儿科和孕妇的临床成像。与基于器官剂量的 ED 相比,基于 DLP 的 ED 可能会高估较大体型患者的有效剂量,低估较小体型患者的有效剂量。