Department of Nephrology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Department of Urology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Clin J Am Soc Nephrol. 2021 Feb 8;16(2):204-212. doi: 10.2215/CJN.10470620. Epub 2021 Jan 27.
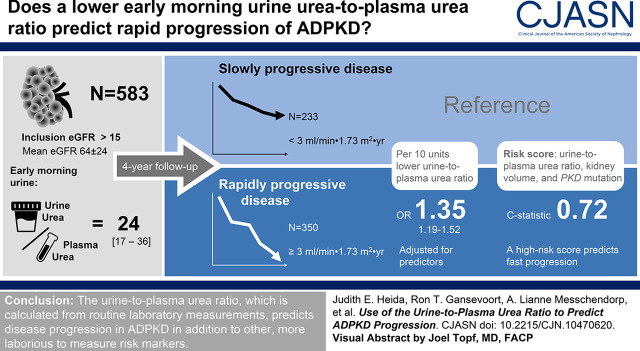
Predicting disease progression in patients with autosomal dominant polycystic kidney disease (ADPKD) poses a challenge, especially in early-stage disease when kidney function is not yet affected. Ongoing growth of cysts causes maximal urine-concentrating capacity to decrease from early on. We therefore hypothesized that the urine-to-plasma urea ratio, as a reflection of the urine-concentrating capacity, can be used as a marker to predict ADPKD progression.
The urine-to-plasma urea ratio was calculated by dividing concentrations of early morning fasting spot urine urea by plasma urea. First, this ratio was validated as surrogate marker in 30 patients with ADPKD who underwent a prolonged water deprivation test. Thereafter, association with kidney outcome was evaluated in 583 patients with ADPKD with a broad range of kidney function. Multivariable mixed-model regression was used to assess association with eGFR slope, and logarithmic regression to identify patients with rapidly progressive disease, using a cutoff of -3.0 ml/min per 1.73 m per year. The urine-to-plasma urea ratio was compared with established predictors, namely, sex, age, baseline eGFR, Mayo Clinic height-adjusted total kidney volume class, and gene mutation.
The maximal urine-concentrating capacity and urine-to-plasma urea ratio correlated strongly (=0.90; <0.001). Next, the urine-to-plasma urea ratio was significantly associated with rate of eGFR decline during a median follow-up of 4.0 (interquartile range, 2.6-5.0) years, both crude and after correction for established predictors (=0.58; =0.02). The odds ratio of rapidly progressive disease was 1.35 (95% confidence interval, 1.19 to 1.52; <0.001) for every 10 units decrease in urine-to-plasma urea ratio, with adjustment for predictors. A combined risk score of the urine-to-plasma urea ratio, Mayo Clinic height-adjusted total kidney volume class, and mutation predicted rapidly progressive disease better than each of the predictors separately.
The urine-to-plasma urea ratio, which is calculated from routine laboratory measurements, predicts disease progression in ADPKD in addition to other risk markers.
This article contains a podcast at https://www.asn-online.org/media/podcast/CJASN/2021_01_27_CJN10470620_final.mp3.
预测常染色体显性多囊肾病(ADPKD)患者的疾病进展具有挑战性,尤其是在肾功能尚未受到影响的早期阶段。囊肿的持续生长导致最大尿浓缩能力从早期开始下降。因此,我们假设尿/血浆尿素比(反映尿浓缩能力)可用作预测 ADPKD 进展的标志物。
尿/血浆尿素比通过将清晨空腹尿液尿素浓度除以血浆尿素浓度来计算。首先,该比值在 30 名接受长时间禁水试验的 ADPKD 患者中作为替代标志物进行了验证。此后,在 583 名具有广泛肾功能的 ADPKD 患者中评估了与肾脏结局的相关性。多变量混合模型回归用于评估与 eGFR 斜率的相关性,对数回归用于确定快速进展性疾病患者,使用 -3.0 ml/min/1.73m/年的截止值。将尿/血浆尿素比与已建立的预测因素(性别、年龄、基线 eGFR、Mayo 临床身高调整的总肾体积类别和 PKD1 基因突变)进行比较。
最大尿浓缩能力和尿/血浆尿素比之间存在很强的相关性(=0.90;<0.001)。接下来,尿/血浆尿素比与中位随访 4.0 年(四分位距 2.6-5.0)期间 eGFR 下降率显著相关,无论是否校正已建立的预测因素(=0.58;=0.02)。尿/血浆尿素比每降低 10 个单位,快速进展性疾病的比值比为 1.35(95%置信区间,1.19-1.52;<0.001),校正预测因素后。尿/血浆尿素比、Mayo 临床身高调整的总肾体积类别和 PKD1 基因突变的组合风险评分预测快速进展性疾病的效果优于每个单独的预测因素。
尿/血浆尿素比(通过常规实验室测量计算得出)除了其他风险标志物外,还可预测 ADPKD 的疾病进展。
本文包含一个播客,网址为 https://www.asn-online.org/media/podcast/CJASN/2021_01_27_CJN10470620_final.mp3。