University of Burgundy-ISITE-BFC-Institut national de la santé et de la recherche médicale (Inserm) UMR1231, Faculty of Medicine, 21079 Dijon, France.
Unit for innovation in genetics and epigenetics in oncology, Dijon University Hospital, 21079 Dijon, France.
Cold Spring Harb Mol Case Stud. 2021 Feb 19;7(1). doi: 10.1101/mcs.a005934. Print 2021 Feb.
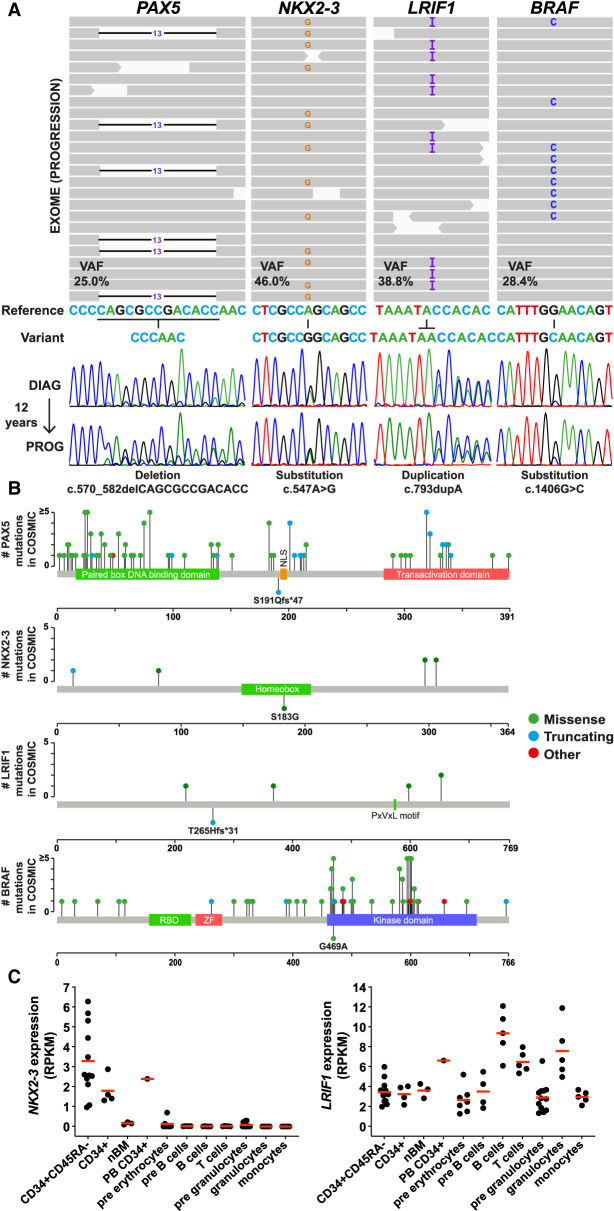
Diagnosis of B-cell chronic lymphocytic leukemia (B-CLL) is usually straightforward, involving clinical, immunophenotypic (Matutes score), and (immuno)genetic analyses (to refine patient prognosis for treatment). CLL cases with atypical presentation (e.g., Matutes ≤ 3) are also encountered, and for these diseases, biology and prognostic impact are less clear. Here we report the genomic characterization of a case of atypical B-CLL in a 70-yr-old male patient; B-CLL cells showed a Matutes score of 3, chromosomal translocation t(14;18)(q32;q21) (), mutated , deletion 17p, and mutations in , (subclonal), and (subclonal). Quite strikingly, a novel mutation that was predicted to be loss of function was also seen. Exome sequencing identified, in addition, a potentially actionable mutation, together with novel somatic mutations affecting the homeobox transcription factor , known to control B-lymphocyte development and homing, and the epigenetic regulator , which is implicated in chromatin compaction and gene silencing. Neither nor mutations, predicted to be loss of function, have previously been reported in B-CLL. Sequencing confirmed the presence of these mutations together with , , and mutations, with the t(14;18)(q32;q21) translocation, in the initial diagnostic sample obtained 12 yr prior. This is suggestive of a role for these novel mutations in B-CLL initiation and stable clonal evolution, including upon treatment withdrawal. This case extends the spectrum of atypical B-CLL with t(14;18)(q32;q21) and highlights the value of more global precision genomics for patient follow-up and treatment in these patients.
B 细胞慢性淋巴细胞白血病(B-CLL)的诊断通常很直接,包括临床、免疫表型(Matutes 评分)和(免疫)遗传学分析(以细化患者的治疗预后)。也会遇到表现不典型的 CLL 病例(例如,Matutes ≤ 3),对于这些疾病,生物学和预后影响尚不明确。在此,我们报告了一例 70 岁男性不典型 B-CLL 病例的基因组特征;B-CLL 细胞的 Matutes 评分为 3,染色体易位 t(14;18)(q32;q21)(),突变,缺失 17p,以及突变在()(亚克隆)、()(亚克隆)和()(亚克隆)中。引人注目的是,还发现了一种预测为功能丧失的新型突变。外显子组测序还鉴定了一种潜在可治疗的突变,以及影响同源盒转录因子的新体细胞突变,该基因已知控制 B 淋巴细胞发育和归巢,以及表观遗传调节剂,其参与染色质紧缩和基因沉默。以前在 B-CLL 中尚未报道过预测为功能丧失的突变和突变。测序证实了这些突变的存在,以及突变、突变和突变,以及在 12 年前获得的初始诊断样本中存在 t(14;18)(q32;q21)易位。这表明这些新突变在 B-CLL 的起始和稳定的克隆进化中发挥作用,包括在治疗停药后。这种情况扩展了具有 t(14;18)(q32;q21)的不典型 B-CLL 的范围,并强调了更全面的精确基因组学在这些患者的患者随访和治疗中的价值。