Monteiro Leonardo L, Skowronski Rodrigo, Brimo Fadi, Carvalho Paulo da C, Vasconcelos Romulo A L, Pacheco Charley R C V, Calado Adriano A, Kassouf Wassim
Division of Urology, McGill University, Montreal, Canada.
Department of Pathology, McGill University, Montreal, Canada.
Int Braz J Urol. 2021 May-Jun;47(3):515-522. doi: 10.1590/S1677-5538.IBJU.2019.0119.
To evaluate the erectile function in patients who underwent partial penectomy and identify factors associated with penile functional status.
We identified patients who underwent partial penectomy due to penile cancer between 2009 and 2014. Clinical and pathological characteristics included patient age at the time of diagnosis, obesity, hypertension, dyslipidemia, diabetes, smoking, metabolic syndrome, Eastern Cooperative Oncology Group (ECOG) status, penile shaft length, tumor size, primary tumor stage (pT), clinical nodal status, and local recurrence. Erectile function was assessed prospectively with the International Index of Erectile Function (IIEF-5) at least 3 months after partial penectomy.
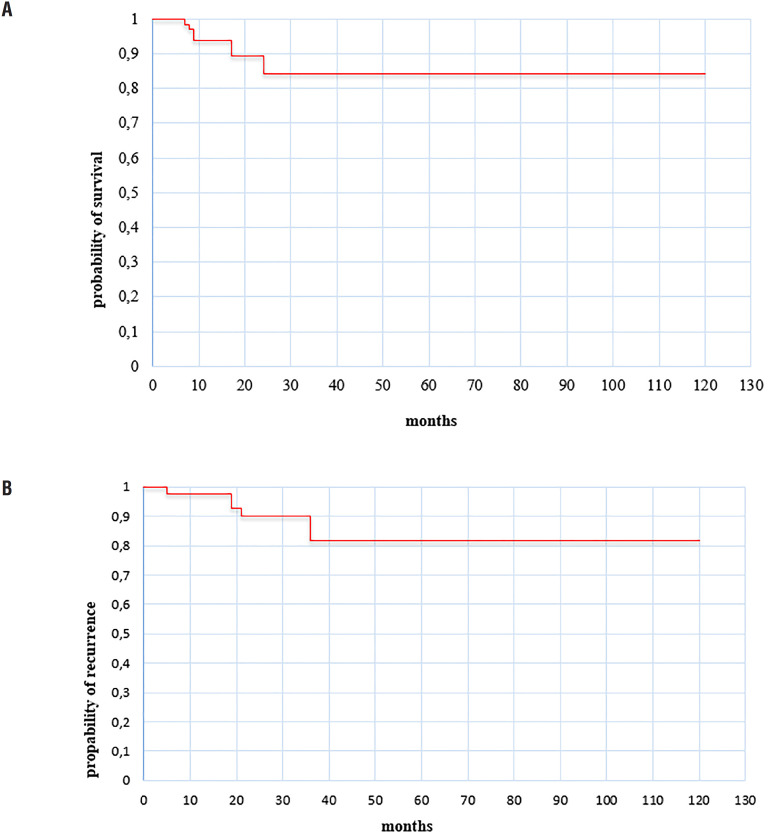
A total of 81 patients met analysis criteria. At the diagnosis, the median age was 62 years (range from 30 to 88). Median follow-up was 17 months (IQR 7-36). Of total patients, 37 (45%) had T2 or higher disease. Clinically positive nodes were present in 16 (20%) patients and seven (8.6%) developed local recurrence. Fifty patients (62%) had erectile dysfunction (ED) after partial penectomy, 30% had moderate or severe erectile dysfunction scores. Patients with ED versus without ED were similar in baseline characteristics except for age, penile shaft length, and presence of inguinal adenopathy (p <0.05). Multivariate analysis using logistic regression confirmed that older patients, shorter penile shaft length, and clinically positive lymph node were significantly associated with ED.
Partial penectomy due to penile cancer provides adequate local control of the disease, however, proper counselling is important especially in relation to ED consequences. Preservation of penile length yields to more optimal erectile recovery.
评估接受部分阴茎切除术患者的勃起功能,并确定与阴茎功能状态相关的因素。
我们纳入了2009年至2014年间因阴茎癌接受部分阴茎切除术的患者。临床和病理特征包括诊断时的患者年龄、肥胖、高血压、血脂异常、糖尿病、吸烟、代谢综合征、东部肿瘤协作组(ECOG)状态、阴茎长度、肿瘤大小、原发肿瘤分期(pT)、临床淋巴结状态和局部复发情况。在部分阴茎切除术后至少3个月,采用国际勃起功能指数(IIEF-5)对勃起功能进行前瞻性评估。
共有81例患者符合分析标准。诊断时,中位年龄为62岁(范围30至88岁)。中位随访时间为17个月(四分位间距7 - 36个月)。在所有患者中,37例(45%)患有T2或更高分期的疾病。16例(20%)患者临床淋巴结阳性,7例(8.6%)发生局部复发。50例(62%)患者在部分阴茎切除术后出现勃起功能障碍(ED),30%患者勃起功能障碍评分为中度或重度。除年龄、阴茎长度和腹股沟淋巴结病外,ED患者与无ED患者的基线特征相似(p<0.05)。使用逻辑回归进行的多因素分析证实,年龄较大、阴茎长度较短和临床淋巴结阳性与ED显著相关。
因阴茎癌进行的部分阴茎切除术可对疾病进行充分的局部控制,然而,尤其是在涉及ED后果方面,进行适当的咨询很重要。保留阴茎长度可实现更理想的勃起功能恢复。