Imperial Vascular Unit, Imperial College London NHS Healthcare Trust, London, UK.
Department of Surgery and Cancer, Imperial College London, London, UK.
Perfusion. 2022 Apr;37(3):276-283. doi: 10.1177/0267659121995760. Epub 2021 Feb 26.
The aim of this study was to identify factors associated with primary graft patency 1 year following open lower limb revascularisation (LLR) at a tertiary referral vascular service.
A retrospective analysis of patients undergoing infra-inguinal bypass surgery between January 2016 and May 2017 at a tertiary vascular centre (St Mary's Hospital, London) was performed. Data regarding patient demographics, comorbidities, type of operation and post-operative anti-thrombotic strategy were collected. Quality of run-off score was assessed from pre-operative imaging.
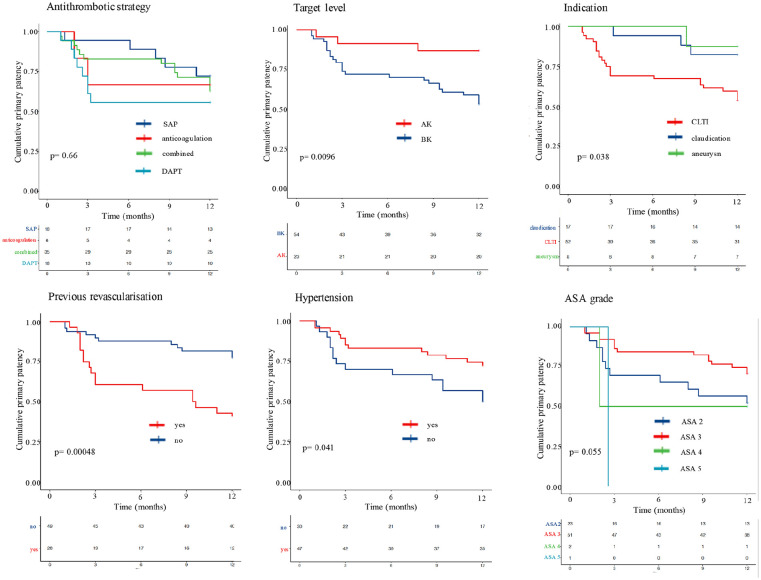
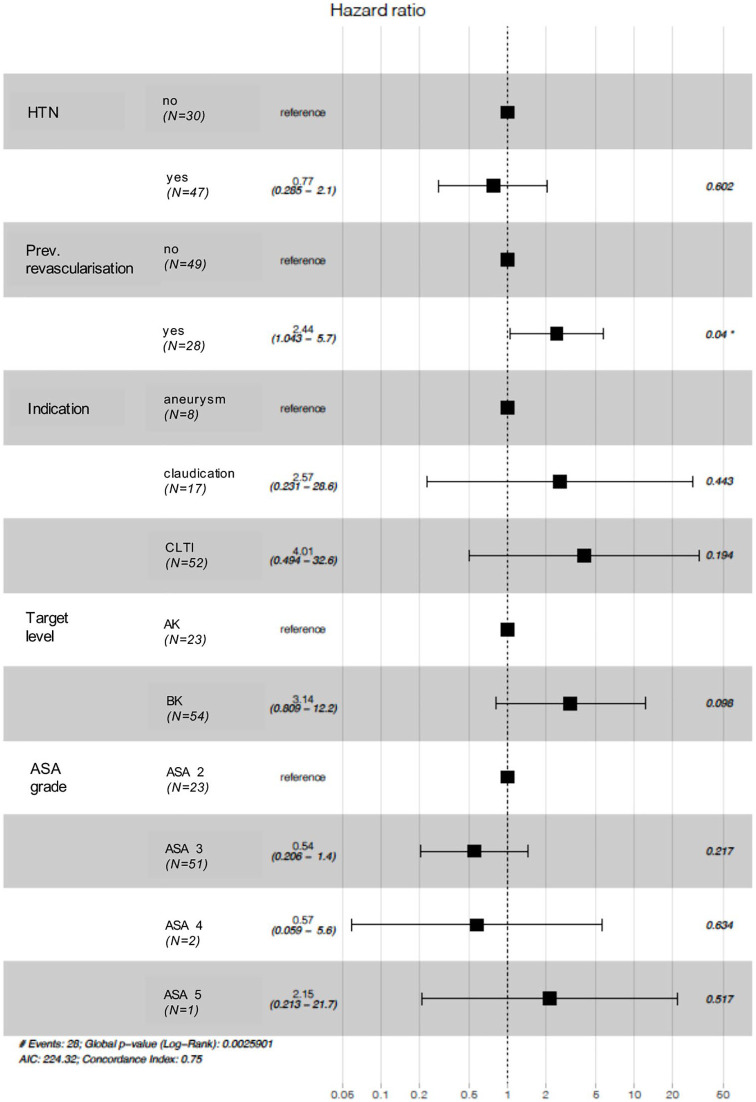
Seventy-seven cases were included in the analysis. Overall, the primary patency rate at 1-year was 63.6% ( = 49/77) and the secondary patency rate was 67.5% ( = 52/77). Independent variables with statistically significant inferior patency rates at 1-year were (1) bypasses with below knee targets (p = 0.0096), (2) chronic limb threatening ischaemia indication (p = 0.038), (3) previous ipsilateral revascularisation (p < 0.001) and (4) absence of hypertension history (p = 0.041). There was also a trend towards significance for American Society of Anesthesiologists (ASA) grade (p = 0.06). Independent variables with log-rank test p values of <0.1 were included in a Cox proportional hazards model. The only variable with a statistically significant impact on primary patency rates was previous open or endovascular ipsilateral revascularisation (HR 2.44 (1.04-5.7), p = 0.04).
At 1-year follow-up, previous ipsilateral revascularisation was the most significant factor in affecting patency rates. Patients in this subgroup should therefore be deemed high-risk, which should be reflected in the informed consent and peri-operative management.
本研究旨在确定在三级转诊血管服务中心进行下肢再血管化(LLR)后 1 年时与主移植物通畅性相关的因素。
对 2016 年 1 月至 2017 年 5 月在三级血管中心(伦敦圣玛丽医院)接受下肢旁路手术的患者进行回顾性分析。收集患者人口统计学、合并症、手术类型和术后抗血栓策略的数据。术前影像学评估评估流出量评分。
共纳入 77 例患者。总体而言,1 年时的主通畅率为 63.6%(49/77),二级通畅率为 67.5%(52/77)。1 年时通畅率统计学上显著降低的独立变量包括:(1)膝下目标的旁路(p=0.0096),(2)慢性肢体威胁性缺血指征(p=0.038),(3)同侧再血管化既往史(p<0.001)和(4)无高血压病史(p=0.041)。美国麻醉师协会(ASA)分级也有显著趋势(p=0.06)。对数秩检验 p 值<0.1 的独立变量纳入 Cox 比例风险模型。对主移植物通畅率有统计学显著影响的唯一变量是同侧既往开放或血管内再血管化(HR 2.44(1.04-5.7),p=0.04)。
在 1 年随访时,同侧再血管化是影响通畅率的最重要因素。因此,该亚组患者应被视为高危患者,这应反映在知情同意书和围手术期管理中。