University of Connecticut School of Pharmacy, 69 North Eagleville Road, Unit 3092, Storrs, CT, 06269, USA.
Evidence-Based Practice Center, Hartford Hospital, Hartford, CT, USA.
Cardiovasc Diabetol. 2021 Feb 26;20(1):52. doi: 10.1186/s12933-021-01250-5.
Diabetes increases a patient's risk of developing atrial fibrillation by 49%. Patients with nonvalvular atrial fibrillation are at a fivefold increased risk of stroke and die more frequently from vascular causes. We sought to evaluate the effectiveness and safety of rivaroxaban versus warfarin in nonvalvular atrial fibrillation patients with type 2 diabetes.
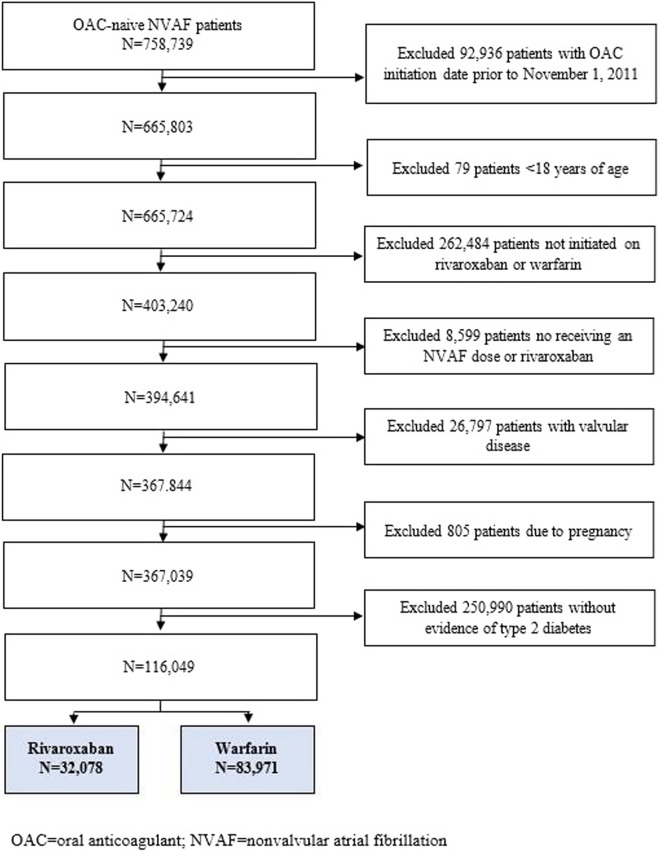
This was an analysis of Optum® De-Identified electronic health record data from 11/2010 to 12/2019. We included adults with nonvalvular atrial fibrillation and type 2 diabetes, newly started on rivaroxaban or warfarin and with ≥ 12-months of prior electronic health record activity. Patients who were pregnant, had alternative indications for oral anticoagulation or valvular heart disease were excluded. We evaluated the incidence rate (%/year) of developing the composite outcome of stroke/systemic embolism or vascular death and major or clinically relevant nonmajor bleeding as well as each endpoint individually. Hazard ratios with 95% confidence intervals were calculated using propensity score-overlap weighted proportional hazards regression.
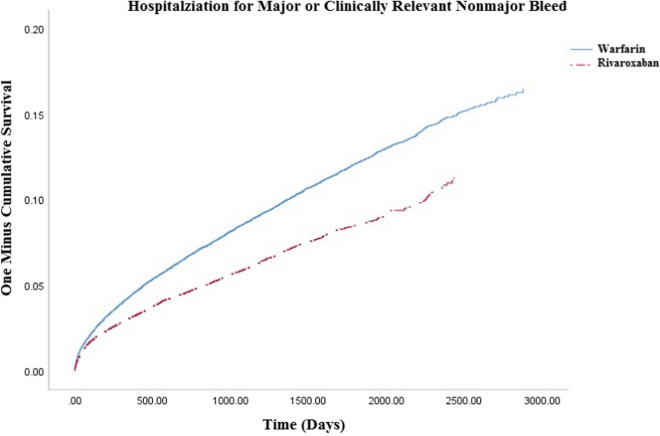
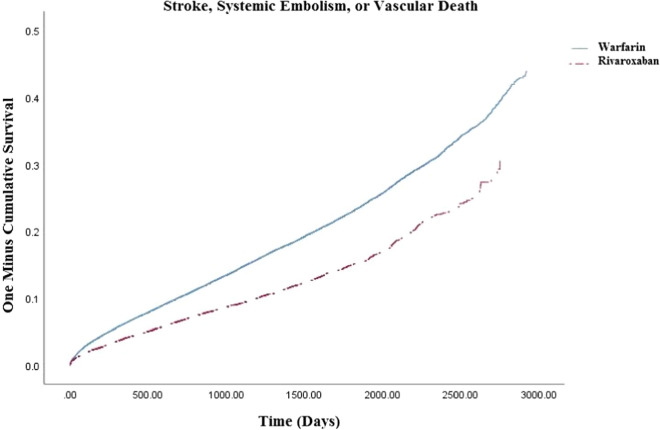
We included 32,078 rivaroxaban (31% initiated on 15 mg dose) and 83,971warfarin users (time-in-therapeutic range = 47 ± 28%). Rivaroxaban was associated with a reduced risk of stroke/systemic embolism or vascular death (3.79 vs. 4.19; hazard ratio = 0.91, 95% confdience interval = 0.88-0.95), driven mostly by reductions in vascular death (2.81 vs 3.18, hazard ratio = 0.90, 95% confidence interval = 0.86-0.95) and systemic embolism (0.13 vs. 0.16; hazard ratio = 0.82, 95% confidence interval = 0.66-1.02). Major/clinically relevant nonmajor bleeding was less frequent with rivaroxaban versus warfarin (2.17 vs. 2.31; hazard ratio = 0.94, 95% confidence interval = 0.89-0.99) due to decreased critical organ bleeding (including intracranial hemorrhage) (0.35 vs. 0.54; hazard ratio = 0.63, 95% confidence interval = 0.55-0.72).
In nonvalvular atrial fibrillation patients with type 2 diabetes, rivaroxaban was associated with an ~ 10% relative reduction in vascular mortality and fewer bleeding-related hospitalizations versus warfarin.
糖尿病使患者发生房颤的风险增加 49%。非瓣膜性房颤患者发生中风的风险增加五倍,死于血管原因的频率更高。我们旨在评估利伐沙班与华法林在 2 型糖尿病合并非瓣膜性房颤患者中的有效性和安全性。
这是一项对 2010 年 11 月至 2019 年 12 月 Optum®去识别电子健康记录数据的分析。我们纳入了新开始使用利伐沙班或华法林且有≥12 个月电子健康记录活动的非瓣膜性房颤合并 2 型糖尿病的成年人。排除了妊娠、有其他口服抗凝剂指征或有瓣膜性心脏病的患者。我们评估了中风/全身性栓塞或血管死亡和主要或临床上相关的非主要出血的复合结局以及每个终点的发生率(%/年)。使用倾向评分重叠加权比例风险回归计算风险比及其 95%置信区间。
我们纳入了 32078 名利伐沙班(31%起始剂量为 15mg)和 83971 名华法林使用者(治疗范围内时间=47±28%)。与华法林相比,利伐沙班降低了中风/全身性栓塞或血管死亡的风险(3.79 比 4.19;风险比=0.91,95%置信区间=0.88-0.95),主要归因于血管性死亡(2.81 比 3.18,风险比=0.90,95%置信区间=0.86-0.95)和全身性栓塞(0.13 比 0.16;风险比=0.82,95%置信区间=0.66-1.02)的减少。与华法林相比,利伐沙班发生主要/临床上相关的非主要出血的频率更低(2.17 比 2.31;风险比=0.94,95%置信区间=0.89-0.99),这是由于关键器官出血(包括颅内出血)减少(0.35 比 0.54;风险比=0.63,95%置信区间=0.55-0.72)。
在合并 2 型糖尿病的非瓣膜性房颤患者中,与华法林相比,利伐沙班使血管性死亡率降低约 10%,并减少与出血相关的住院治疗。