Makower Della, Lin Juan, Xue Xiaonan, Sparano Joseph A
Montefiore Einstein Center for Cancer Care, Bronx, NY, USA.
Albert Einstein Cancer Center, Bronx, NY, USA.
NPJ Breast Cancer. 2021 Mar 1;7(1):20. doi: 10.1038/s41523-021-00231-x.
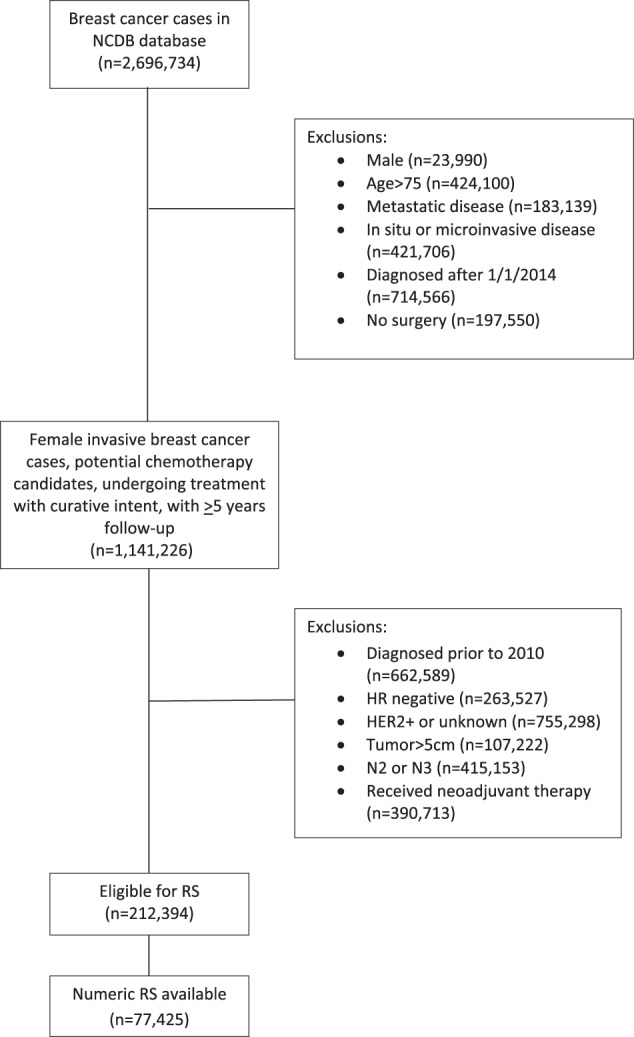
Lymphovascular invasion (LVI) and Black race are associated with poorer prognosis in early breast cancer (EBC). We evaluated the association between LVI and race, and whether LVI adds prognostic benefit to the 21-gene recurrence score (RS) in EBC. Women with ER+ HER2- EBC measuring up to 5 cm, with 0-3 involved axillary nodes, diagnosed between 1 January 2010 and 1 January 2014, who underwent surgery as first treatment and had available RS, were identified in the NCDB database. Bivariate associations between two categorical variables were examined using chi-square test. Multivariate Cox proportional hazards model were used to assess the association of LVI, race, and other covariates with overall survival (OS). 77,425 women, 65,018 node-negative (N0), and 12,407 with 1-3 positive (N+) nodes, were included. LVI was present in 12.7%, and associated with poor grade, RS 26-100, and N+ (all p < 0.0001), but not Black race. In multivariate analysis, LVI was associated with worse OS in N0 [HR 1.37 (95% CI 1.27, 1.57], but not N+ EBC. LVI was associated with worse OS in N0 patients with RS 11-25 [HR 1.31 (95% CI 1.09, 1.57)] and ≥26 [HR 1.58 (95% CI 1.30, 1.93)], but not RS 0-10. No interaction between LVI and chemotherapy benefit was seen. Black race was associated with worse OS in N0 (HR 1.21, p = 0.009) and N+ (HR 1.37, p = 0.015) disease. LVI adds prognostic information in ER+, HER2-, N0 BCA with RS 11-100, but does not predict chemotherapy benefit. Black race is associated with worse OS, but not LVI.
淋巴管浸润(LVI)和黑人种族与早期乳腺癌(EBC)的预后较差相关。我们评估了LVI与种族之间的关联,以及LVI是否能为EBC的21基因复发评分(RS)增加预后价值。在国家癌症数据库(NCDB)中确定了2010年1月1日至2014年1月1日期间诊断的ER + HER2- EBC患者,肿瘤最大径达5cm,腋窝淋巴结转移0 - 3个,接受手术作为首次治疗且有可用RS的患者。使用卡方检验检查两个分类变量之间的双变量关联。多变量Cox比例风险模型用于评估LVI、种族和其他协变量与总生存期(OS)的关联。共纳入77425名女性,其中65018名淋巴结阴性(N0),12407名有1 - 3个阳性淋巴结(N +)。LVI发生率为12.7%,与低分级、RS 26 - 100和N +相关(所有p < 0.0001),但与黑人种族无关。在多变量分析中,LVI与N0患者的OS较差相关[风险比(HR)1.37(95%置信区间[CI] 1.27, 1.57)],但与N + EBC无关。LVI与RS 11 - 25 [HR 1.31(95% CI 1.09, 1.57)]和≥26 [HR 1.58(95% CI 1.30, 1.93)]的N0患者的OS较差相关,但与RS 0 - 10无关。未观察到LVI与化疗获益之间的相互作用。黑人种族与N0(HR 1.21,p = 0.009)和N +(HR 1.37,p = 0.015)疾病的OS较差相关。LVI可为RS 11 - 100的ER +、HER2 -、N0乳腺癌增加预后信息,但不能预测化疗获益。黑人种族与较差的OS相关,但与LVI无关。