Experimental Developmental Therapeutics (EDT) Program, Mays Cancer Center at UT Health MD Anderson, San Antonio, Texas, USA.
Department of Urology, UT Health San Antonio, San Antonio, Texas, USA.
J Immunother Cancer. 2021 Mar;9(3). doi: 10.1136/jitc-2020-001941.
Although intravesical BCG is the standard treatment of high-grade non-muscle invasive bladder cancer (NMIBC), response rates remain unsatisfactory. In preclinical models, rapamycin enhances BCG vaccine efficacy against tuberculosis and the killing capacity of γδ T cells, which are critical for BCG's antitumor effects. Here, we monitored immunity, safety, and tolerability of rapamycin combined with BCG in patients with NMIBC.
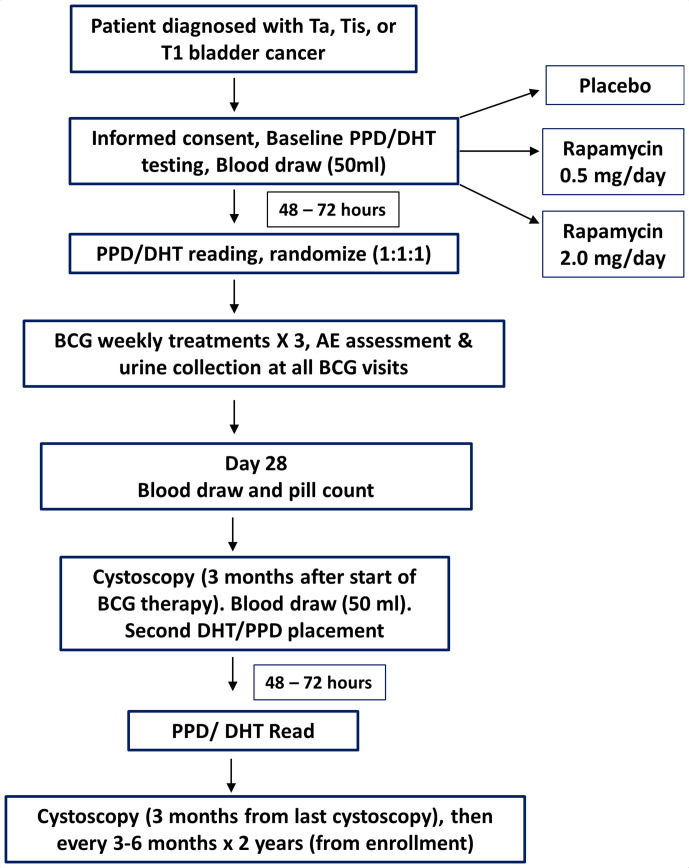
A randomized double-blind trial of oral rapamycin (0.5 or 2.0 mg daily) versus placebo for 1 month was conducted in patients with NMIBC concurrently receiving 3 weekly BCG instillations (NCT02753309). The primary outcome was induction of BCG-specific γδ T cells, measured as a percentage change from baseline. Post-BCG urinary cytokines and immune cells were examined as surrogates for local immune response in the bladder. Secondary outcomes measured were adverse events (AEs) and tolerability using validated patient-reported questionnaires.
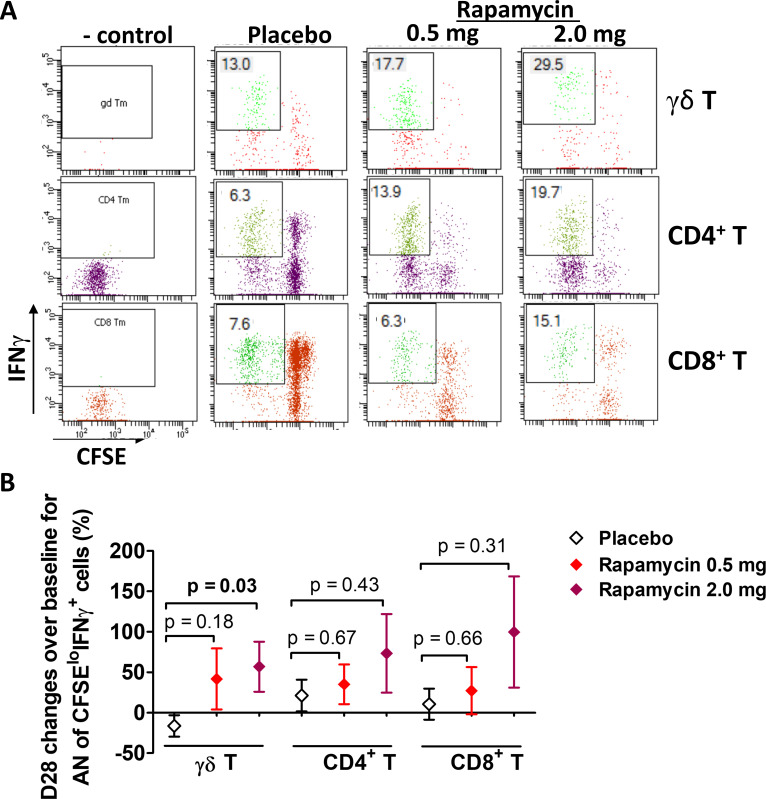
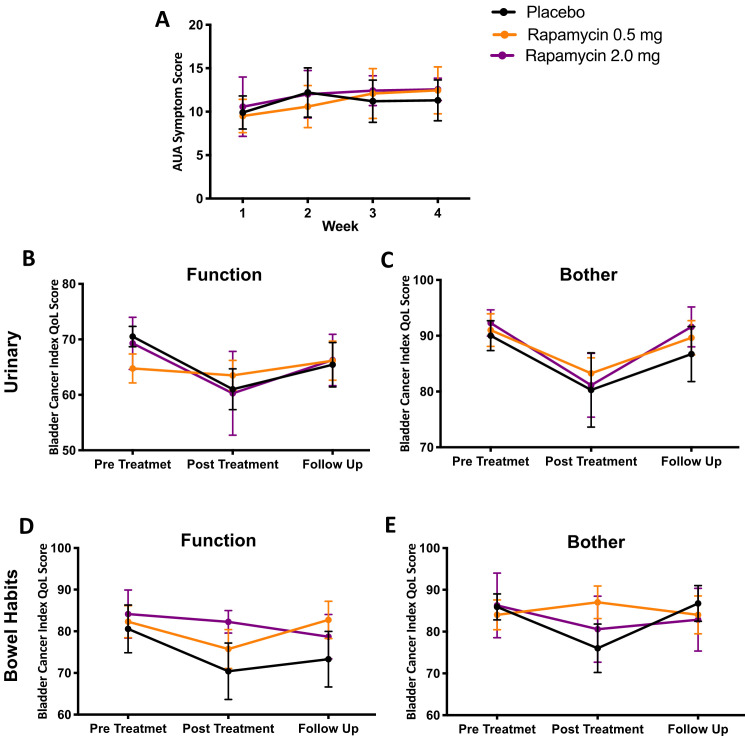
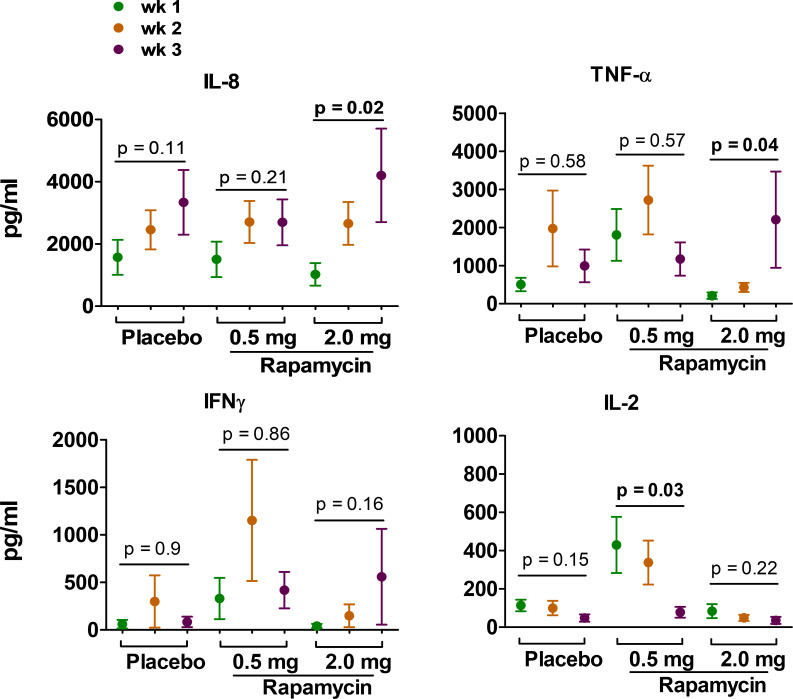
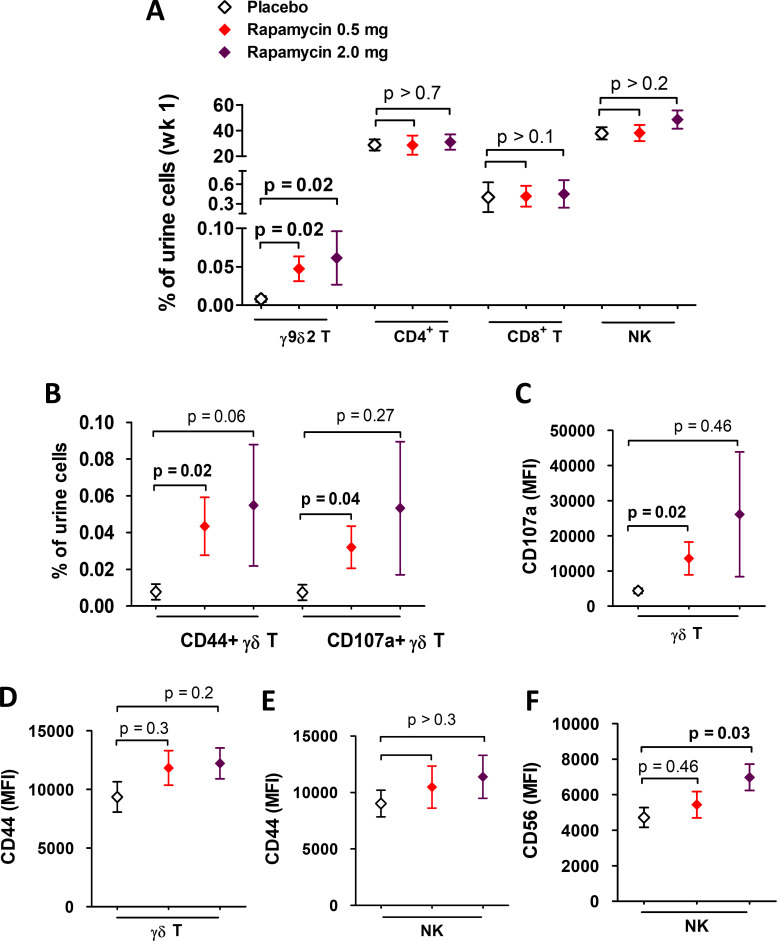
Thirty-one patients were randomized (11 placebo, 8 rapamycin 2.0 mg, and 12 rapamycin 0.5 mg). AEs were similar across groups and most were grade 1-2. One (12.5%) patient randomized to 2.0 mg rapamycin was taken off treatment due to stomatitis. No significant differences in urinary symptoms, bowel function, or bother were observed between groups. The median (IQR) percentage change in BCG-specific γδ T cells from baseline per group was as follows: -26% (-51% to 24%) for placebo, 9.6% (-59% to 117%) for rapamycin 0.5 mg (versus placebo, p=0.18), and 78.8% (-31% to 115%) for rapamycin 2.0 mg (versus placebo, p=0.03). BCG-induced cytokines showed a progressive increase in IL-8 (p=0.02) and TNF-α (p=0.04) over time for patients on rapamycin 2.0 mg, whereas patients receiving placebo had no significant change in urinary cytokines. Compared with placebo, patients receiving 2.0 mg rapamycin had increased urinary γδ T cells at the first week of BCG (p=0.02).
Four weeks of 0.5 and 2.0 mg oral rapamycin daily is safe and tolerable in combination with BCG for patients with NMIBC. Rapamycin enhances BCG-specific γδ T cell immunity and boosts urinary cytokines during BCG treatment. Further study is needed to determine long-term rapamycin safety, tolerability and effects on BCG efficacy.
虽然膀胱内卡介苗(BCG)是治疗高级别非肌肉浸润性膀胱癌(NMIBC)的标准治疗方法,但反应率仍不理想。在临床前模型中,雷帕霉素增强了卡介苗疫苗对结核的疗效和 γδ T 细胞的杀伤能力,这对 BCG 的抗肿瘤作用至关重要。在这里,我们监测了雷帕霉素联合 BCG 在 NMIBC 患者中的免疫、安全性和耐受性。
一项随机、双盲、平行对照研究,在接受 3 次每周 BCG 膀胱内灌注的同时,口服雷帕霉素(0.5 或 2.0mg/天)或安慰剂治疗 1 个月(NCT02753309)。主要结局是通过与基线相比的百分比变化来测量 BCG 特异性 γδ T 细胞的诱导。BCG 后尿液细胞因子和免疫细胞被作为膀胱局部免疫反应的替代物进行检测。次要结局是使用经过验证的患者报告问卷评估不良事件(AE)和耐受性。
31 名患者被随机分配(11 名安慰剂,8 名雷帕霉素 2.0mg,12 名雷帕霉素 0.5mg)。各组之间的 AE 相似,大多数为 1-2 级。1 名(12.5%)随机接受 2.0mg 雷帕霉素的患者因口炎停止治疗。各组之间的尿症状、肠道功能和困扰均无显著差异。各组从基线开始的 BCG 特异性 γδ T 细胞的中位数(IQR)百分比变化如下:安慰剂组为-26%(-51%至 24%),雷帕霉素 0.5mg 组为 9.6%(-59%至 117%)(与安慰剂相比,p=0.18),雷帕霉素 2.0mg 组为 78.8%(-31%至 115%)(与安慰剂相比,p=0.03)。BCG 诱导的细胞因子显示,接受 2.0mg 雷帕霉素的患者的 IL-8(p=0.02)和 TNF-α(p=0.04)随时间逐渐增加,而接受安慰剂的患者尿液细胞因子无明显变化。与安慰剂相比,接受 2.0mg 雷帕霉素的患者在 BCG 的第一周时尿液 γδ T 细胞增加(p=0.02)。
在 NMIBC 患者中,每天口服 0.5 和 2.0mg 雷帕霉素联合 BCG 4 周是安全且耐受的。雷帕霉素增强了 BCG 特异性 γδ T 细胞免疫,并在 BCG 治疗期间增强了尿液细胞因子。需要进一步研究以确定雷帕霉素的长期安全性、耐受性和对 BCG 疗效的影响。