Yakabe Daisuke, Fukuyama Yusuke, Araki Masahiro, Nakamura Toshihiro
Department of Cardiology Clinical Research Institute National Hospital Organization Kyushu Medical Center Fukuoka City Japan.
J Arrhythm. 2021 Jan 4;37(1):79-87. doi: 10.1002/joa3.12492. eCollection 2021 Feb.
The low voltage zone (LVZ) detected with three-dimensional electroanatomical mapping is a surrogate marker of atrial scar in patients with persistent atrial fibrillation (PeAF) and is associated with poor clinical outcomes after catheter ablation. However, fewer studies have reported the relationship between responsiveness to antiarrhythmic drugs and the LVZ.
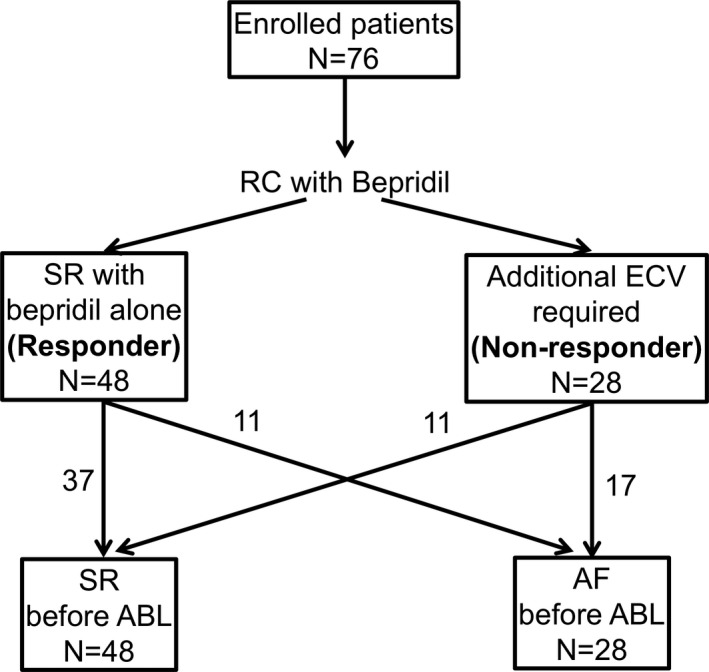
We retrospectively analyzed 76 patients who underwent catheter ablation for PeAF at our center. Rhythm control with bepridil was initiated before ablation in all patients, and electrical cardioversion was performed in cases of failure to restore sinus rhythm with bepridil alone. Patients with successful sinus restoration with bepridil alone (≤200 mg/d) were defined as "responders", while those who required electrical cardioversion as well were defined as "non-responders". We compared the LVZ ratio (ratio of the LVZ surface area to the left atrium surface area on three-dimensional electroanatomical mapping) and the recurrence-free rate after ablation between the two groups.
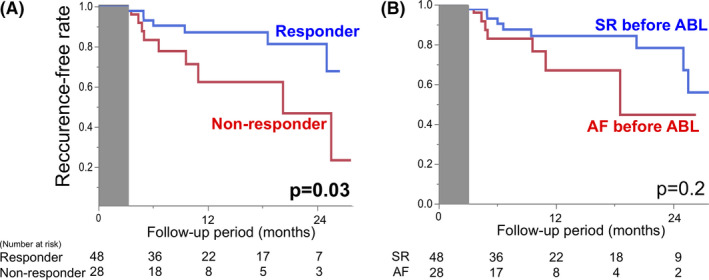
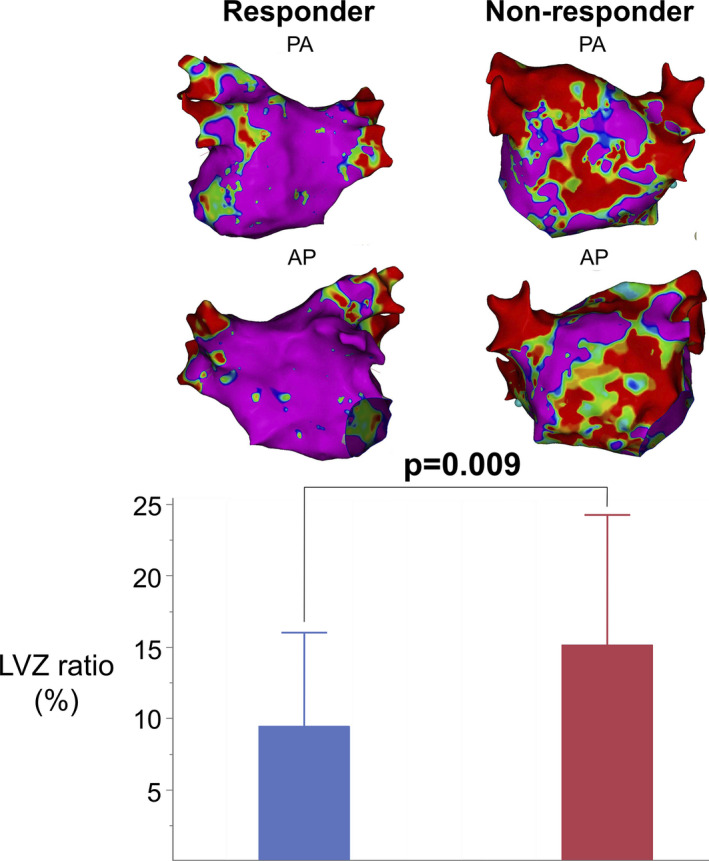
Of the 76 patients, 48 (63.2%) were responders to bepridil. The median LVZ ratio was significantly lower in the responder group than in the nonresponder group (7.5% vs 14.0%, = .009). Multivariate analysis revealed that response to bepridil was an independent predictor of normal voltage ( = .02, odds ratio = 0.20, 95% confidence interval = 0.04-0.76). The recurrence-free rate at 1 year after catheter ablation was significantly higher in the responder group than in the nonresponder group (87.1% vs 62.3%, = .03).
Response to bepridil is a marker of normal voltage in electroanatomical mapping and is significantly associated with better clinical outcomes after catheter ablation.
三维电解剖标测检测到的低电压区(LVZ)是持续性房颤(PeAF)患者心房瘢痕的替代标志物,并且与导管消融术后不良临床结局相关。然而,较少有研究报道抗心律失常药物反应性与LVZ之间的关系。
我们回顾性分析了在我们中心接受PeAF导管消融的76例患者。所有患者在消融前开始使用苄普地尔进行节律控制,对于单独使用苄普地尔未能恢复窦性心律的患者进行电复律。单独使用苄普地尔(≤200mg/d)成功恢复窦性心律的患者被定义为“反应者”,而那些还需要电复律的患者被定义为“无反应者”。我们比较了两组之间的LVZ比率(三维电解剖标测上LVZ表面积与左心房表面积的比率)以及消融后的无复发率。
在76例患者中,48例(63.2%)对苄普地尔有反应。反应者组的LVZ比率中位数显著低于无反应者组(7.5%对14.0%,P = 0.009)。多变量分析显示,对苄普地尔的反应是正常电压的独立预测因素(P = 0.02,比值比 = 0.20,95%置信区间 = 0.04 - 0.76)。导管消融术后1年的无复发率在反应者组显著高于无反应者组(87.1%对62.3%,P = 0.03)。
对苄普地尔的反应是电解剖标测中正常电压的标志物,并且与导管消融术后更好的临床结局显著相关。