Daubin Cédric, Fournel François, Thiollière Fabrice, Daviaud Fabrice, Ramakers Michel, Polito Andréa, Flocard Bernard, Valette Xavier, Du Cheyron Damien, Terzi Nicolas, Fartoukh Muriel, Allouche Stephane, Parienti Jean-Jacques
Department of Medical Intensive Care, CHU de Caen, 14000, Caen, France.
Department of Biostatistics and Clinical Research, CHU de Caen, 14000, Caen, France.
Ann Intensive Care. 2021 Mar 6;11(1):39. doi: 10.1186/s13613-021-00816-6.
To assess the ability of procalcitonin (PCT) to distinguish between bacterial and nonbacterial causes of patients with severe acute exacerbation of COPD (AECOPD) admitted to the ICU, we conducted a retrospective analysis of two prospective studies including 375 patients with severe AECOPD with suspected lower respiratory tract infections. PCT levels were sequentially assessed at the time of inclusion, 6 h after and at day 1, using a sensitive immunoassay. The patients were classified according to the presence of a documented bacterial infection (including bacterial and viral coinfection) (BAC + group), or the absence of a documented bacterial infection (i.e., a documented viral infection alone or absence of a documented pathogen) (BAC- group). The accuracy of PCT levels in predicting bacterial infection (BAC + group) vs no bacterial infection (BAC- group) at different time points was evaluated by receiver operating characteristic (ROC) analysis.
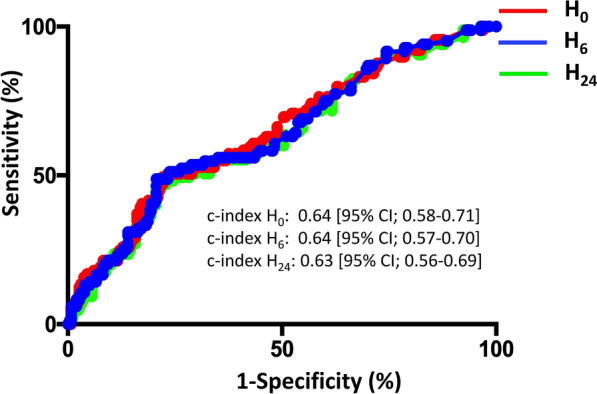
Regarding the entire cohort (n = 375), at any time, the PCT levels significantly differed between groups (Kruskal-Wallis test, p < 0.001). A pairwise comparison showed that PCT levels were significantly higher in patients with bacterial infection (n = 94) than in patients without documented pathogens (n = 218) (p < 0.001). No significant difference was observed between patients with bacterial and viral infection (n = 63). For example, the median PCT-H levels were 0.64 ng/ml [0.22-0.87] in the bacterial group vs 0.24 ng/ml [0.15-0.37] in the viral group and 0.16 ng/mL [0.11-0.22] in the group without documented pathogens. With a c-index of 0.64 (95% CI; 0.58-0.71) at H, 0.64 [95% CI 0.57-0.70] at H and 0.63 (95% CI; 0.56-0.69) at H, PCT had a low accuracy for predicting bacterial infection (BAC + group).
Despite higher PCT levels in severe AECOPD caused by bacterial infection, PCT had a poor accuracy to distinguish between bacterial and nonbacterial infection. Procalcitonin might not be sufficient as a standalone marker for initiating antibiotic treatment in this setting.
为评估降钙素原(PCT)区分入住重症监护病房(ICU)的慢性阻塞性肺疾病急性加重期(AECOPD)患者细菌感染与非细菌感染病因的能力,我们对两项前瞻性研究进行了回顾性分析,这两项研究共纳入375例疑似下呼吸道感染的重症AECOPD患者。在纳入时、6小时后及第1天,使用灵敏的免疫测定法依次评估PCT水平。根据是否存在确诊的细菌感染(包括细菌和病毒合并感染)(BAC+组)或不存在确诊的细菌感染(即仅确诊病毒感染或不存在确诊病原体)(BAC-组)对患者进行分类。通过受试者工作特征(ROC)分析评估不同时间点PCT水平预测细菌感染(BAC+组)与无细菌感染(BAC-组)的准确性。
对于整个队列(n = 375),在任何时间,各组间PCT水平均有显著差异(Kruskal-Wallis检验,p < 0.001)。两两比较显示,细菌感染患者(n = 94)的PCT水平显著高于无确诊病原体患者(n = 218)(p < 0.001)。细菌和病毒合并感染患者(n = 63)之间未观察到显著差异。例如,细菌组的PCT-H中位数水平为0.64 ng/ml [0.22 - 0.87],病毒组为0.24 ng/ml [0.15 - 0.37],无确诊病原体组为0.16 ng/mL [0.11 - 0.22]。在H时c指数为0.64(95%CI;0.58 - 0.71),在H时为0.64 [95%CI 0.57 - 0.70],在H时为0.63(95%CI;0.56 - 0.69),PCT预测细菌感染(BAC+组)的准确性较低。
尽管细菌感染导致的重症AECOPD患者PCT水平较高,但PCT区分细菌感染与非细菌感染的准确性较差。在这种情况下,降钙素原作为启动抗生素治疗的单一标志物可能并不充分。