Department of Vascular Medicine, Amsterdam Cardiovascular Sciences, Amsterdam UMC, University of Amsterdam, Amsterdam, the Netherlands.
Department of Internal Medicine & Radboud Institute of Health Sciences (RIHS, Radboud University Medical Center, Nijmegen, the Netherlands.
J Thromb Haemost. 2021 May;19(5):1174-1185. doi: 10.1111/jth.15290. Epub 2021 Mar 26.
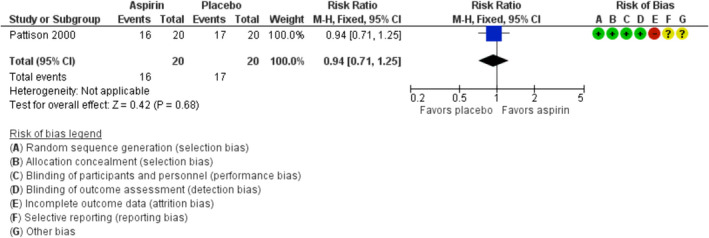
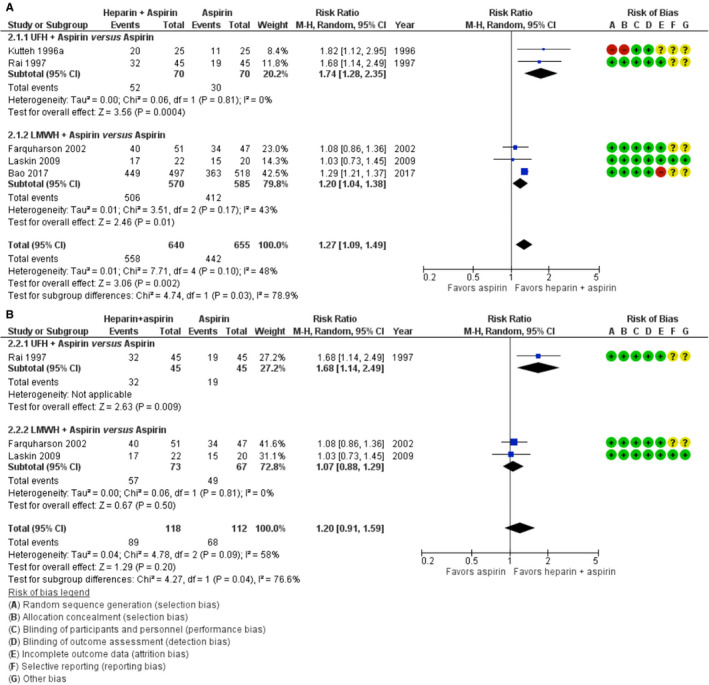
Aspirin and heparin are widely used to reduce the risk of recurrent pregnancy loss in women with antiphospholipid syndrome. This practice is based on only a few intervention studies, and uncertainty regarding benefits and risk remains. In this case-based review, we summarize the available evidence and address the questions that are most important for clinical practice. We performed a systematic review of randomized controlled trials assessing the effect of heparin (low molecular weight heparin [LMWH] or unfractionated heparin [UFH]), aspirin, or both on live birth rates in women with persistent antiphospholipid antibodies and recurrent pregnancy loss. Eleven trials including 1672 women met the inclusion criteria. Aspirin only did not increase live birth rate compared to placebo in one trial of 40 women (risk ratio [RR] 0.94; 95% confidence interval [CI] 0.71-1.25). One trial of 141 women reported a higher live birth rate with LMWH only than with aspirin only (RR 1.20; 95% CI 1.00-1.43). Five trials totaling 1295 women compared heparin plus aspirin with aspirin only. The pooled RR for live birth was 1.27 (95% CI 1.09-1.49) in favor of heparin plus aspirin. There was significant heterogeneity between the subgroups of LMWH and UFH (RR for LWMH plus aspirin versus aspirin 1.20, 95% CI: 1.04-1.38; RR for UFH plus aspirin versus aspirin 1.74, 95% CI: 1.28-2.35; I 78.9%, p = .03). Characteristics of participants and adverse events were not uniformly reported. Heparin (LMWH or UFH) plus aspirin may improve live birth rates in women with recurrent pregnancy loss and antiphospholipid antibodies, but evidence is of low certainty.
阿司匹林和肝素广泛用于降低抗磷脂综合征妇女复发性妊娠丢失的风险。这种做法仅基于少数干预研究,其益处和风险仍存在不确定性。在本次基于病例的综述中,我们总结了现有证据,并针对对临床实践最重要的问题进行了讨论。我们系统地回顾了评估肝素(低分子肝素 [LMWH] 或未分馏肝素 [UFH])、阿司匹林或两者联合应用对持续性抗磷脂抗体和复发性妊娠丢失妇女活产率影响的随机对照试验。11 项试验共纳入 1672 名妇女,符合纳入标准。一项纳入 40 名妇女的试验发现,与安慰剂相比,单独使用阿司匹林并未增加活产率(风险比 [RR] 0.94;95%置信区间 [CI] 0.71-1.25)。一项纳入 141 名妇女的试验报告称,单独使用 LMWH 的活产率高于单独使用阿司匹林(RR 1.20;95% CI 1.00-1.43)。5 项共纳入 1295 名妇女的试验比较了肝素联合阿司匹林与单独使用阿司匹林。肝素联合阿司匹林与单独使用阿司匹林相比,活产率的汇总 RR 为 1.27(95% CI 1.09-1.49),对肝素联合阿司匹林有利。LMWH 和 UFH 的亚组之间存在显著异质性(LMWH 联合阿司匹林与阿司匹林相比的 RR 为 1.20,95% CI:1.04-1.38;UFH 联合阿司匹林与阿司匹林相比的 RR 为 1.74,95% CI:1.28-2.35;I² = 78.9%,p = 0.03)。参与者特征和不良事件的报告并不统一。肝素(LMWH 或 UFH)联合阿司匹林可能会提高复发性妊娠丢失和抗磷脂抗体妇女的活产率,但证据的确定性较低。