Chapot René, Stracke Christian Paul, Wallocha Marta, Rikhtegar Reza, Yamac Elif, Mosimann Pascal John
Department of Intracranial Endovascular Therapy, Alfried Krupp Krankenhaus Essen, Essen, Germany
Department of Intracranial Endovascular Therapy, Alfried Krupp Krankenhaus Essen, Essen, Germany.
J Neurointerv Surg. 2022 Feb;14(2):160-163. doi: 10.1136/neurintsurg-2021-017279. Epub 2021 Mar 15.
Self-expanding stents are increasingly being deployed for stent-assisted coiling or flow diversion of intracranial aneurysms. Complications related to stent misbehavior may arise, however, including lack of expansion, device displacement, or parent vessel thrombosis. We present our experience of various stent removal techniques (stentectomy) with a focus on technical and clinical outcomes.
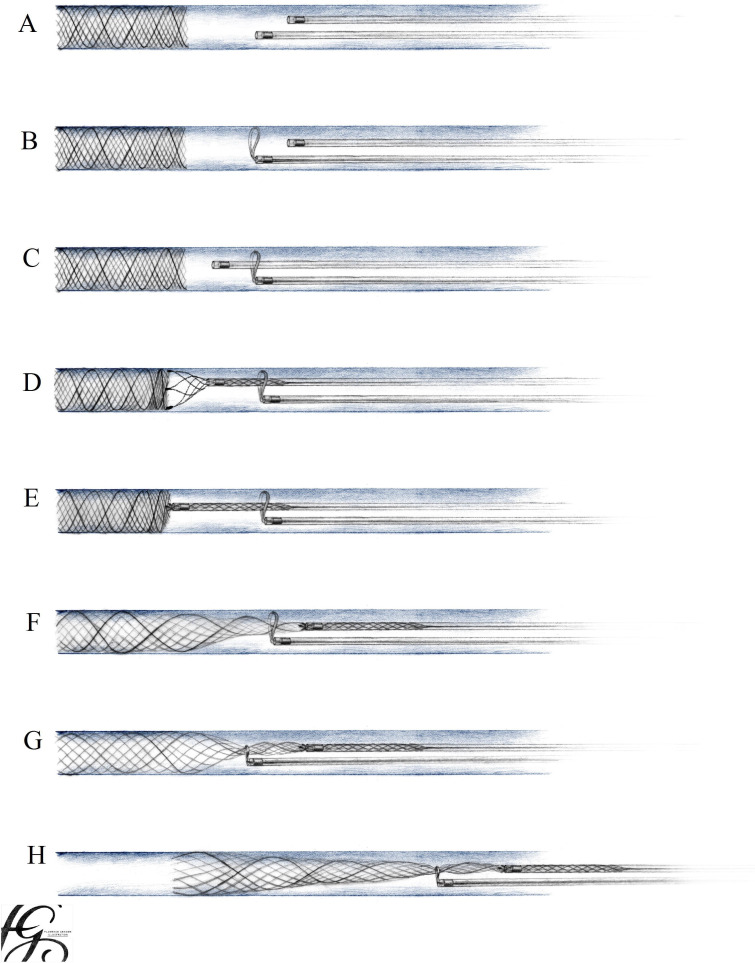
Stentectomy was attempted either with a single device, including the Alligator, Microsnare, or Solitaire, or by combining a Microsnare with a second device. Dual techniques included in this report are the Snare-over-Stentretriever technique we developed using a Microsnare and a Solitaire, and the previously described Loop-and-Snare technique using a Microsnare and a microwire. The technical success and complication rate, as well as the clinical outcome using the mRS were analyzed.
Forty-seven stentectomies were attempted in 36 patients treated for 37 aneurysms. Forty-two devices (89.3%) were successfully retrieved. Single-device stentectomy was successful in 34% of cases, compared with 74% with dual-device techniques. Of the 20 patients with a thrombosed parent or efferent vessel, 17 were successfully recanalized using stentectomy. All successful stentectomy patients made a clinically uneventful recovery, except one with a minor postoperative stroke (mRS 1 at discharge). Failed stentectomy was associated with major ischemic stroke in two patients and death in one patient. There were no stentectomy-related vessel perforations or dissections.
While various single devices can be used to safely retrieve dysfunctional intracranial self-expandable stents, dual-device techniques are more than twice as effective, according to our experience.
自膨式支架越来越多地用于颅内动脉瘤的支架辅助弹簧圈栓塞或血流导向治疗。然而,可能会出现与支架功能异常相关的并发症,包括扩张不全、装置移位或载瘤血管血栓形成。我们介绍了各种支架取出技术(支架切除术)的经验,重点关注技术和临床结果。
尝试使用单一器械进行支架切除术,包括鳄嘴钳、微型圈套器或Solitaire支架取栓器,或通过将微型圈套器与第二种器械联合使用。本报告中包括的双重技术是我们使用微型圈套器和Solitaire支架取栓器开发的圈套器套在支架取栓器上的技术,以及先前描述的使用微型圈套器和微导丝的圈套器联合技术。分析了技术成功率、并发症发生率以及使用改良Rankin量表(mRS)评估的临床结果。
对36例治疗37个动脉瘤的患者尝试进行了47次支架切除术。成功取出42个器械(89.3%)。单器械支架切除术在34%的病例中成功,而双器械技术的成功率为74%。在20例载瘤或流出血管血栓形成的患者中,17例通过支架切除术成功再通。除1例术后出现轻度卒中(出院时mRS为1)外,所有成功进行支架切除术的患者临床恢复均顺利。支架切除术失败与2例患者发生严重缺血性卒中和1例患者死亡相关。未发生与支架切除术相关的血管穿孔或夹层。
根据我们的经验,虽然各种单一器械可用于安全取出功能失调的颅内自膨式支架,但双器械技术的有效性是单一器械技术的两倍多。