Center for Medical Ethics and Health Policy, Baylor College of Medicine, One Baylor Plaza MC: 420, Houston, TX, 77030, USA.
Division of Heart Failure, Houston Methodist Hospital, Smith Tower, 6550 Fannin St., Ste 1901, Houston, TX, 77030, USA.
BMC Med Inform Decis Mak. 2021 Mar 20;21(1):106. doi: 10.1186/s12911-021-01468-z.
A central goal among researchers and policy makers seeking to implement clinical interventions is to identify key facilitators and barriers that contribute to implementation success. Despite calls from a number of scholars, empirical insights into the complex structural and cultural predictors of why decision aids (DAs) become routinely embedded in health care settings remains limited and highly variable across implementation contexts.
We examined associations between "reach", a widely used indicator (from the RE-AIM model) of implementation success, and multi-level site characteristics of nine LVAD clinics engaged over 18 months in implementation and dissemination of a decision aid for left ventricular assist device (LVAD) treatment. Based on data collected from nurse coordinators, we explored factors at the level of the organization (e.g. patient volume), patient population (e.g. health literacy; average sickness level), clinician characteristics (e.g. attitudes towards decision aid; readiness for change) and process (how the aid was administered). We generated descriptive statistics for each site and calculated zero-order correlations (Pearson's r) between all multi-level site variables including cumulative reach at 12 months and 18 months for all sites. We used principal components analysis (PCA) to examine any latent factors governing relationships between and among all site characteristics, including reach.
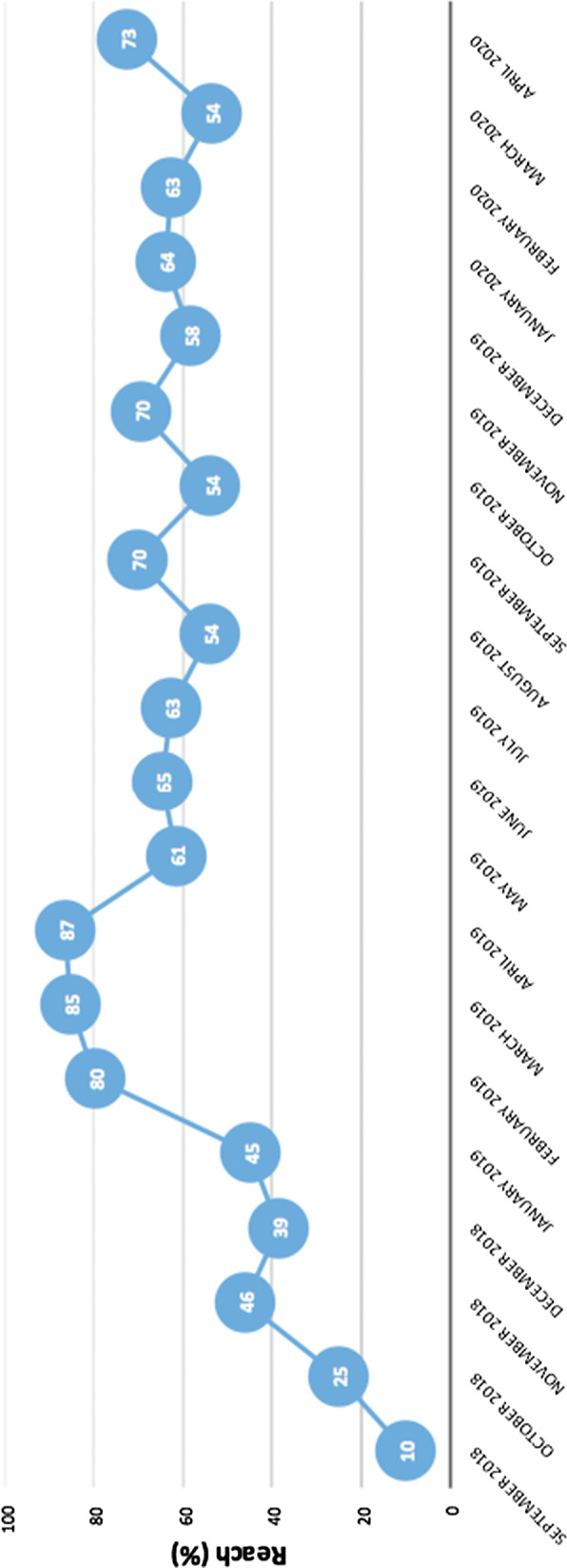
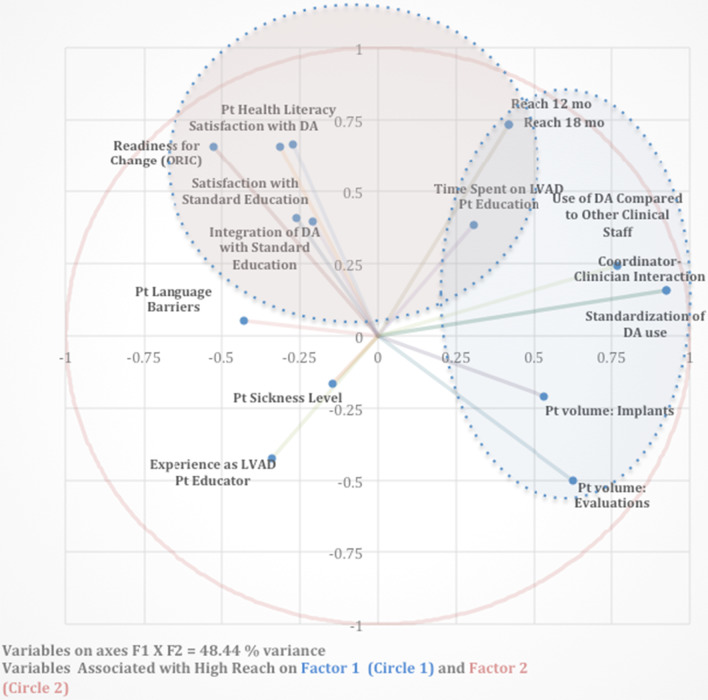
We observed strongest inclines in reach of our decision aid across the first year, with uptake fluctuating over the second year. Average reach across sites was 63% (s.d. = 19.56) at 12 months and 66% (s.d. = 19.39) at 18 months. Our PCA revealed that site characteristics positively associated with reach on two distinct dimensions, including a first dimension reflecting greater organizational infrastructure and standardization (characteristic of larger, more established clinics) and a second dimension reflecting positive attitudinal orientations, specifically, openness and capacity to give and receive decision support among coordinators and patients.
Successful implementation plans should incorporate specific efforts to promote supportive and mutually informative interactions between clinical staff members and to institute systematic and standardized protocols to enhance the availability, convenience and salience of intervention tool in routine practice. Further research is needed to understand whether "core predictors" of success vary across different intervention types.
寻求实施临床干预的研究人员和政策制定者的一个核心目标是确定有助于实施成功的关键促进因素和障碍。尽管有许多学者呼吁,但对于决策辅助工具(DA)为何会成为医疗保健环境中常规工具的复杂结构和文化预测因素的实证见解仍然有限,并且在实施背景下高度可变。
我们研究了“可及性”(RE-AIM 模型中的一个广泛使用的指标)与 9 个 LVAD 诊所的多层次站点特征之间的关联,这些诊所参与了 18 个月的左心室辅助装置(LVAD)治疗决策辅助工具的实施和传播。根据从护士协调员收集的数据,我们探讨了组织层面的因素(例如患者数量)、患者人群(例如健康素养;平均疾病水平)、临床医生特征(例如对决策辅助工具的态度;变革准备)和流程(辅助工具的管理方式)。我们为每个站点生成了描述性统计数据,并计算了所有站点 12 个月和 18 个月的累积可及性与所有多层次站点变量之间的零阶相关性(皮尔逊 r)。我们使用主成分分析(PCA)来检查控制所有站点特征之间关系的任何潜在因素,包括可及性。
我们观察到我们的决策辅助工具的可及性在第一年急剧上升,第二年的使用率波动不定。所有站点的 12 个月和 18 个月的平均可及性分别为 63%(标准差=19.56)和 66%(标准差=19.39)。我们的 PCA 显示,与可及性相关的站点特征在两个不同维度上呈正相关,包括反映更大的组织基础设施和标准化的第一维度(反映更大、更成熟的诊所的特征),以及反映积极的态度取向的第二维度,具体而言,协调员和患者之间的决策支持的开放性和接受能力。
成功的实施计划应包括具体努力,以促进临床工作人员之间的支持性和相互信息交流,并建立系统和标准化的协议,以提高干预工具在常规实践中的可用性、便利性和突出性。需要进一步研究以了解不同干预类型的成功“核心预测因素”是否存在差异。